J.ophthalmol.(Ukraine).2022;4:68-74.
|
http://doi.org/10.31288/oftalmolzh202246874 Received: 20.06.2022; Accepted: 18.07.2022; Published on-line: 24.08.2022 Neuropsychological diagnostics and correction of reading disorders in visually impaired children M. K. Kremenchutska, O. L. Kiparenko, L. D. Chykur, V. V. Pundiev, I. V. Dobrynina Odesa I. I. Mechnikov National University; Odesa (Ukraine)
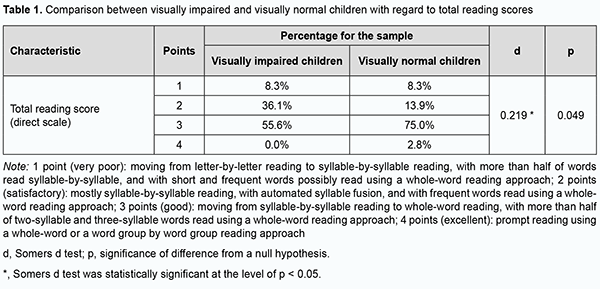
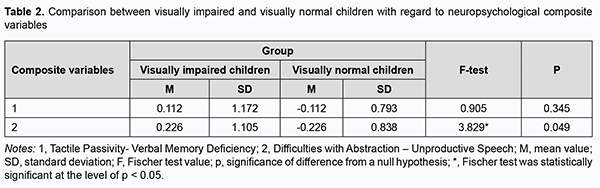
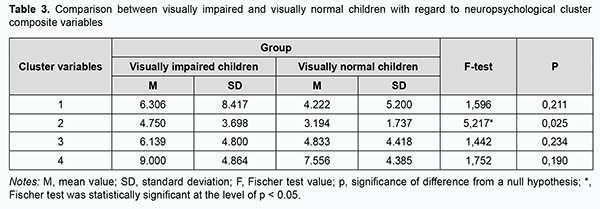
TO CITE THIS ARTICLE: Kremenchutska MK, Kiparenko OL, Chykur LD, Pundiev VV, Dobrynina IV. Neuropsychological diagnostics and correction of reading disorders in visually impaired children. J.ophthalmol.(Ukraine).2022;4:68-74. From year to year, there has been an increase in the number of children with poor reading skills. The paper focuses on a neuropsychological approach to assessing reading learning difficulties in visually impaired children. Purpose: To examine the impact of neuropsychological characteristics on reading learning difficulties in visually impaired children. Material and Methods: The study sample included 72 children aged 8-12 years; of these, 36 had a vision impairment. We used a battery of neuropsychological tests proposed by Luria and adapted for children by Glozman. Statistical analysis was conducted using IBM SPSS Statistics 23 software. Results: There was a significant difference (p < 0.05) in neuropsychological test results between the experimental group and controls. The neuropsychological symptom complex (cluster) for visually impaired children comprises certain markers of regulation and control like Difficulties in Memorizing a Series of Elements, Difficulties in Retaining Semantic Elements of a Text, Immaturity of Holistic Reading, Slow Reading, Impossibility to Make a Program for an Arithmetic Problem, Difficulties in Naming the Found Category, and Situational Generalization. Conclusion: It was found that the degree of the maturity of neuropsychological characteristics (regulation mechanisms) in the domains of motor and intellectual functioning has an effect on learning difficulties in reading in visually impaired children. Understanding the neuropsychological mechanisms of reading disorders in visually impaired children has a key value for neuropsychological differential diagnosis with subsequent correct identification of targets for neuropsychological correction. Keywords: reading disorders, dyslexia, neuropsychological diagnostics, neuropsychological correction, visually impaired children, difficulties in regulation and control Introduction From year to year, there has been an increase in the number of children with poor reading skills, with the impairment affecting their self-esteem and mental development [1-4]. Most commonly, parents of schoolchildren with learning difficulties visit a neuropsychologist because of the child’s learning difficulties in writing and reading and/or difficulties in concentrating. The aforementioned difficulties at school reflect deficient morphological and functional genesis, and not all symptoms of these difficulties are early noted by parents, medical professionals, neuropsychologists and speech therapists. Difficulties of learning and adaptation at school are most commonly based on the factor of asynchronous development of cognitive functions. This results in (a) an immaturity (delay) of mental functions such as digital and hand praxis (performing purposeful movements and actions), visual-spatial orientation, speed of proceeding and the volume of memorization of verbal and motor information, and regulation, and (b) sensory information-processing deficiency [5, 6]. Along with a decrease in the rate of success at school, there has been observed a decrease in the rate of visual acuity loss in school pupils, especially in junior school pupils. Sometimes parents note that their child needs to examine objects (like letters or digits) at near, rubs his/her eyes, complains of headache and his/her eyes get tired quickly from writing and/or reading. This results in visiting an ophthalmologist and having vision correction. Studies have demonstrated an association of reduced visual acuity with increased time spent with computers, cell phones, handheld video games, and other electronic devices, particularly, for children. Falkenverg and colleagues [7] demonstrated changes in the vision status in primary and secondary schoolchildren aged 7-15 years referred from vision screening during the 10 year period of 2003-2013. Foreman and colleagues [8] reviewed the literature on the association between digital smart device use and myopia. Our experience has shown that parents of schoolchildren frequently associate the child’s learning difficulties in reading with visual problems. General reading disorders in children may be temporary (in the presence of some external factors) or permanent. There are two distinct forms of reading disorder in children: a difficulty in learning to translate print into speech and reading comprehension impairment [9]. Dyslexia is defined as a sustained failure to learn reading or difficulties with learning reading, when intelligence and physical capacity to hear are not at issue [10]. In addition, dyslexia may be classified into two main categories, phonological (or auditory) dyslexia and visual dyslexia, with most reading errors referred to these two categories [10]. Dyslexia has been studied by researchers from different fields of study like medicine, speech therapy and psychology [9]. Different explanatory, diagnostic and remedial approaches to dyslexia have been proposed. Studies (including clinical ones) vary in definitions of dyslexia, with these definitions including diverse and sometimes inconsistent abnormalities and origins of these abnormalities. Therefore, in matters of dyslexia, there are diverse points of views and various approaches with sometimes fuzzy definitions, causes and methods of correction. Approaches to treatment of dyslexic children with vision impairments are commonly focused on achieving improvements in reading skills through improvements in the quality of vision. Functional Magnetic Resonance Imaging (fMRI) studies have demonstrated that there is no linear relationship between the development of reading skills and occipital and temporal lobes, with the functions of secondary occipital and temporal regions associated with auditory and visual signal processing [11]. Considering the contribution to our understanding of neuropsychological abnormalities in children by the Luria’s neuropsychological theory, Glozman and colleagues reviewed the effects of an increase in the level of formation of neuropsychological factors with an increase in child’s age on difficulties in mastering reading skills (a technique of text reading and comprehension). Glozman presented a neuropsychological approach to reading learning difficulties, the technique being focused on the comprehensive explanation of psychological, genetic and neurological bases for mechanisms of reading [12]. The structure of the neuropsychological method is based on Luria’s factor analysis theory. According to this theory, functional systems of a human body have common links, or components, in their mechanism. Therefore, the presence of a primary defect associated with a function of a particular brain region inevitably results in an impairment in several functional systems. Such a method systemically approaches any functional abnormalities for diagnostics and subsequent correction of the problem. Specialists from the Center for Practical Neuropsychology (Odesa) have conducted a study that demonstrates the structure of the defect on the basis of associations of brain structure and function with mental processes. The purpose of this study was to examine the impact of maturity of neuropsychological characteristics on acquisition of reading skills by children with vision impairments. Material and Methods The study sample included 72 children aged 8-12 years whose parents sought neuropsychological evaluation at the Center for Practical Neuropsychology (Odesa) from October, 2021, to December, 2021. The child’s difficulties with reading at school were a major cause for seeking professional help. Children were divided into two groups. Group 1 was composed of 36 children with vision impairments, with the most common impairments being astigmatism, myopia, allergic conjunctivitis, and spasm of accommodation [13, 14]. Group 2 (the control group) was composed of 36 children offering no complaints of vision, and was matched with regard to age and gender to group 1. Of the 36 children, 4 (11%) were 8 years old; 8 (22%), 9 years old; 9 (25%), 10 years old; 9 (25%), 11 years old; and 6 (17%), 12 years old. No comorbidity was observed in any child. We conducted a neuropsychological assessment using a battery of neuropsychological tests proposed by Luria, adapted for children by Glozman [15] to reveal the causes and the mechanism of difficulties in learning at school. The methodology was translated into Ukrainian and adapted for conducting studies in Ukraine [16]. Each child was assessed individually in the presence of his/her parents. Parents were sitting or standing as observers at some distance behind the child. The examination procedure was about 60 minutes long and included a 5-minute break. Praxis (purposeful movements and actions) tests, dynamic praxis test and digital praxis tests were also used as a break [15]. Luria’s battery of neuropsychological tests adapted for children [17] is used to reveal the causes and the mechanism of difficulties in learning at school. The results of neuropsychological assessment allow singling out neuropsychological correction targets and assigning priorities to these targets in a particular case [15]. The brevity of the methodology is an important advantage for a single screening assessment of the child’s higher mental functions and zone of proximal development, with this assessment being limited by time. All the tests are differentiated by age and may be re-performed as needed. The neuropsychological assessment includes assessments of the following domains: General characteristics of the child, Mental neurodynamics, Motor functions, Gnosis, Speech, Memory, and Reasoning. There are different types of errors related to each of the above domains, with a particular neuropsychological factor underlying this or that error [15, 17]. The initial steps of the child assessment procedure are the tasks focused on the energy component of mental activity (tests for neurodynamics, auditory and verbal memory and attention requiring functional involvement of subcortical brain structures). Two similar tasks (e.g., two intelligence tests) are not performed sequentially. Univariate analysis of variance (ANOVA) and hierarchical cluster analysis using Ward's method [18] were performed for statistical analysis using IBM SPSS Statistics 23 software. All binary neuropsychological characteristics were treated as cluster objects. The children under examination were viewed as cluster parameters. A dendrogram (cluster analysis tree) reflects the results of object grouping at each step of the algorithm. The procedure is a method for reducing data dimension to investigate the internal structure of the examined system of a certain number of variates. Principal component analysis (PCA) analyzes a data table representing observations that are described by several dependent variables that are inter-correlated and allows the extraction of important information from the table to represent it as a new set of orthogonal variables called principal components. Clustering algorithms include hierarchical clustering, in which similarity between observations may be represented on a dendrogram. Results The results of neuropsychological tests in children with vision impairments (the experimental group) and in those with no vision impairment (the control group) were assessed for dissimilarity using the Cramer-Welch test. Some neuropsychological characteristics were significantly lower in children with a vision disorder. There was a significant difference between groups in the following 12 characteristics: Difficulties in Memorizing a Series of Elements (p = 0.001), Difficulties in Retaining Semantic Elements of a Text (p = 0.013), Kinesthetic Difficulties (p = 0.034), Untidy and Oversimplified Drawing (p = 0.046), Synkinesis (p = 0.018), Ignorance of a Portion of the Tactile Space While Touching with Fingers of Both Hands (p = 0.032), Immature Letter Formation (p = 0.020), Monotonous Reading (p = 0.031), Perseverations, Kinesthetic Changes in Reading/Writing (p = 0.032), Poor Knowledge of Orthographic Rules (p = 0.006), Impulsivity in Analyzing a Picture or a Story (p = 0.016), and Impossibility to Make a Program for a Problem (p = 0.001). Of the above 12 characteristics, eight (i.e., most) are related to regulatory functions. Reading problems were the focus of our attention, because it was for these problems that professional help was sought. Frequency analysis of a Total Reading Score for the control and experimental groups was performed. Somers d test was used to assess the association between Total Reading Score and the experimental group. At the next stage of the study, the method of principal components was used to consider associations between neuropsychological parameters to generalize empirical data. We decided to develop a two-principal component solution which can be easily visualized in a two-dimensional space. The first two principal components explained 26.707% of the total variance. The initial solution was rotated to an oblique simple structure (Promax, k = 4). Since the number of components was rather high (more than one hundred), we will review the most significant of them. The first component had a positive pole (defined by the Inactive Touching variable) and a negative pole (defined by the Failure of Memorizing Semantic Elements of Text variable), and was named Tactile Passivity- Verbal Memory Deficiency. The second component had a positive pole (defined by the Difficulties in Naming the Found Category variable) and a negative pole (defined by the Impulsivity, Verbalism, Mannerism in Speech variable), and was named Difficulties with Abstraction – Unproductive Speech. Component values were saved in separate integral variables obtained by regression, in order to make subsequent component analysis easier. Consequently, measures of central tendency were close to 0, with a standard deviation close to 1. Univariate analysis of variance (ANOVA) was used to consider differences in integral component variables between visually impaired and visually normal children. There was a statistically significant difference (p < 0.050) in the second component variable between the two groups, i.e., Difficulties with Abstraction were more characteristic for visually impaired children. These are primarily difficulties in voluntary regulation and control of mental activity, and visually impaired children exhibit difficulties with generalization of texts which cause difficulties in intelligent understanding of the text. In addition, we considered the way in which certain neuropsychological symptoms cluster to form a “symptom complex”. With this in mind, the centroids of neuropsychological characteristics were grouped within the data space of the two components. A large number of neuropsychological characteristics enabled us using Ward's agglomerative hierarchical clustering method, with the squared Euclidean distance used as a similarity measure [19]. All binary neuropsychological characteristics were treated as cluster objects. The children under examination were viewed as cluster parameters. The cluster analysis tree was produced and cluster characteristics were defined. The number of variables included in the analysis was 100. The four-cluster model showed a significant leap in the agglomeration coefficient. Cluster 1 included the following variables: Low Productivity of Memorizing (V1), Increased Trace Inhibition (V2), Inactivity of Learning (“plateau”) (V4), Confabulations (V6), Perseverations (V7), Phonetic Substitutions (V9), Perceptual Substitutions (Visually Similar Image) (V13), Difficulties in Retaining Motor Program (V14), A Need for Tips for Reproducing the Learnt Motor Program (V15), Low Intellectual Performance (V16), Low Concentration of Attention (V17), Distraction from the Job (V21), General Retardation and Aspontaneity (V22), Impulsivity in Motor Tests (V25), Inertia (V28), Dysautomatized (sporadic) Movements (V29), Systemic Perseverations (V43), Immaturity of Visual Gnosis (Object Recognition) (V45), Impulsivity in Gnostic Tests (V46), Pseudoagnosia (V49), Ignorance of One Side of the Visual Space (V50), Inactivity (V55), Ignorance of a Portion of the Tactile Space While Touching with Fingers of Both Hands (V57), Inactivity of Touching (V58), Prosodic Disturbances (V60), Dysphonia or Low Voice (V61), Disturbed Fluency (“Chopped” Speech) (V62), Poor Speech (V63), Verbal and Literal Paraphasias (V64), Agrammatisms: Misuse of Prepositions, Endings, Erroneous Words Concordance (V65), Search of Names for Objects and Paraphasias in Naming (V66), Inertia (Perseverations) in Naming (V67), Difficulties in Understanding the Instructions (V69), Constriction of Speech Perception Volume (V70), Poor Vocabulary (V72), Perseverations and Kinesthetic Substitutions in Writing and Reading (V77), Inattention to Sentence and Phrase Markers (Point, Capital Letter, Comma, etc.) (V78), Unstable Word Image (V79), Poor Knowledge of Orthographic Rules (V81), Impulsivity, Verbalism, Mannerism in Speech (V86), Inability to Understand the Pictured Story (V87), Slow Understanding, Need for Tips (V88), Misunderstanding the Digit Position of a Number (V91), Aspontaneity in Intellectual Activity (V95), and Inertia in Tasks for Generalization or Grasping the Analogies (V97). Cluster 2 included the following variables: Fluctuations in the Amount of Learning (V3), Difficulty in Memorizing a Series of Elements (V8), Exhaustibility in Memorizing (V11), Difficulties in Retaining Semantic Elements of a Text (V12), Immature Selective Attention (V20), Loss of Program in Reaction Selection Test (V24), Micrographia in the Graphic Test for Dynamic Praxis (V31), Untidy and Oversimplified Drawing (V34), Tension, Slowness in Reciprocal Coordination (V36), Extra Impulses when Reproducing Rhythmic Structures (V41), Difficulties in Speech Motor Control (V42), Immature Acoustic Gnosis (Overestimation of Rhythm) (V51), Immature Acoustic Gnosis (Underestimation of Rhythm) (V52), Immature Tactile Gnosis (V56), Immature Letter Formation (V59), Immaturity of Holistic Reading (V73), Slow Reading (V74), Micrographia in Writing (V82), Impossibility to Make a Program for an Arithmetic Problem (V94), Difficulties in Naming the Found Category (V98), and Situational Generalization (V100). Cluster 3 included the following variables: Stereotypes in Dynamic Praxis (V27), Macrographia (V32), Alternative or Symmetric Movements in Reciprocal Coordination (V37), Ignorance of One Hand in Reciprocal Coordination (V39), General Motor Clumsiness (V44), Fragmentation of Perception (V47), Difficulties of Simultaneous Synthesis in Perception (V48), Weakness of Acoustic Attention (V53), Immaturity of Phonemic Hearing (V68), Regulatory Defects Despite Knowledge of the Orthographic Rules (V80), Macrographia, Uneven Handwriting and Increased Muscle Tone when Writing (V83), Inaccurate Writing (V84), Non-retention of a Line when Writing (V85), Impulsivity when Analyzing a Picture or a Story (V89), Forgetting the Intermediate Result in Calculation (V92), Perseverations in Calculation (V93), and Immaturity of Generalization and Logical Connection Establishing Processes (V99). Cluster 4 included the following variables: Difficulty of Starting Memorization (Low Level after the First Presentation) (V5), Semantic Substitutions (V10), Fluctuations in Intellectual Capacity (V18), Exhaustion (V19), Difficulty to Start the Test (V23), A Simplification of the Program for Dynamic Praxis (V26), Kinesthetic Difficulties (V30), Difficulties in Spatial Organization of Movements and Actions (V33), Compensatory Pushing Arms Sideward in Reciprocal Coordination (V35), Incomplete Fist Closure in Reciprocal Coordination (V38), Synkinesis (V40), Errors in Perception of Spatial Characteristics of Visual Stimuli (V54), Difficulties in Understanding the Logical–Grammatical Relations (V71), Guessing Reading (V75), Monotonous Reading (V76), Non-automatized Calculation (V90), and Impulsive Decision in Tasks (V96). The absence of a characteristic was coded 0 and presence of a characteristic was coded 1. A score for a cluster was calculated by summing up points for all variables included in the cluster. As a result, a composite variable was created for each of the clusters. Univariate analysis of variance (ANOVA) was used to consider differences in composite variables between visually impaired and visually normal children. There was a significant difference in the cluster 2 composite variable between visually impaired and visually normal children. The features related to difficulties in voluntary regulation of mental activity were more characteristic for visually impaired children. Discussion Our principal component analysis demonstrated that the features of the Difficulties with Abstraction pole were more characteristic for visually impaired children and not characteristic for visually normal children with learning difficulties in reading. Visually impaired children exhibit difficulties with generalization of texts which causes difficulties in intelligent understanding of the text. The groups of neuropsychological characteristics that were grouped together within the space of this component may be interpreted as clustering of certain neuropsychological symptoms to form a neuropsychological symptom complex. Most of the neuropsychological characteristics found are related to a deficiency in the third functional unit of the brain, indicating immaturity of child’s regulatory functions. Cluster 2 of the clusters found in the current study contains the variables more typical for visually impaired children, with ten of these variables related to difficulties in maturation of voluntary regulation and control of the child’s mental activity. The 10 variables were the most numerous group among others. Difficulties in regulation and control were the focus of subsequent correction activities. According to Luria's concept of functional units of the brain, the third unit is located in the frontal lobes, anterior to the anterior central central and is responsible for programming, regulating, and verifying conscious mental activity. In individuals with immature frontal lobes, one can observe the processes influencing the course of all mental functions, because they are involved in activity regulation, closely associated with cortical movement regulation, and have an impact on gnostic and mnestic processes as well as intellectual abilities [16]. The results of the current study demonstrate that, in children with eye diseases like astigmatism, myopia, allergic conjunctivitis, and spasm of accommodation, not only the problems of processing visual information (i.e., the problems related to partial deficiency in the occipital cortical regions of the second functional unit) usually indicated by parents and teachers can affect learning quality. This deficiency is reflected in Cluster 2 by “Immature Letter Formation”, which affects the child’s reading skills. But the main thing that the cluster analysis revealed was the predominance of regulatory problems (i.e., the problems related to deficiency in the preanterior regions of the third functional unit) in children with reading difficulties. This deficiency is reflected primarily by Immature Selective Attention, Loss of Program in Reaction Selection Test, and Simplification of the Program for Dynamic Praxis. Parents of visually impaired children usually focus on the child’s medical supervision when facing difficulties in child’s learning (particularly, learning difficulties in reading). Visual impairment can affect exteroreceptive information processing, but, in many cases, is not a prime cause of learning difficulties. Regulation-related targets for correction should be determined either solely by parents or by parents with a neuropsychologist. Correct and detailed instructions from a neuropsychologist will facilitate an improvement in the child’s voluntary self-regulation. Correction will be effective if emotional involvement of the child is adequate and if playful techniques are used. The child will gradually confine his/her impulsive behavior to the task in hand while obeying the rules of the game. Correction interventions should be aimed at developing attention skills in a child to facilitate an improvement in concentration required for performance of appropriate tasks. The first part of correction program should include a set of games and exercises (motor tasks and intellectual tasks [20]) for the formation of regulatory and control functions in the child. The exercises in this part of the program are designed to help the formation of motor coordination, selective attention and attention switching skills and promote impulsivity control. The second part of correction program should include a set of games and exercises for developing thinking as a higher mental function, with special attention to the formation of generalization process in the child. The activities of the second part of correction program should help not only overcoming reading and comprehension difficulties, but also forming a positive attitude to reading. These activities may involve those aimed at improving verbal attention, forming letter and word images, boosting letter recognition speed, and enlarging the child’s vocabulary, and analyze-and-compare and sample activities.
Conclusion
It was found that the degree of the maturity of neuropsychological characteristics (regulation mechanisms) in the domains of motor and intellectual functioning has an effect on learning difficulties in reading in visually impaired children. Understanding the neuropsychological mechanisms of poor reading in visually impaired children has a key value for neuropsychological differential diagnosis with subsequent correct identification of targets for neuropsychological correction. References 1.Caqueo-Urízar A, Mena-Chamorro P, Atencio-Quevedo D, Flores J, Urzúa A. Self-esteem in adolescents with learning difficulties: A study from the perspective of the students, parents, and teachers. Psychology in the Schools. 2021; 10 (58):2031-2040. 2.Medvedovska NV. Results of the study on the impact of eye disease on child quality of life. J Ophthalmology (Ukraine). 2021; 6:48-51. 3.Coelho VA, Marchante M, Jimerson SR. Promoting a Positive Middle School Transition: A Randomized-Controlled Treatment Study Examining Self-Conceptand Self-Esteem. J Youth Adolescence. 2017; 46:558–569. 4.Atowa UC, Hansraj R, Wajuihian SO. Visual problems: a review of prevalence studies on visual impairment in school-age children. Int J Ophthalmol. 2019; 12(6):1037-1043. 5.Kiparenko OL. [Sensory integration as a method of correction of disorders in children]. Problemy suchasnoi psykholohii. 2020; 49:152-176. Ukrainian. 6.Nielsen AN, Brand F, La Cour A. Exploration of Sensory Processing Difficulties among Children Attending Primary School in Denmark. Occup Ther Int. 2021 Mar 24;2021:8893345. 7.Falkenberg HK, Langaas T, Svarverud E. Vision status of children aged 7–15 years referred from school vision screening in Norway during 2003–2013: a retrospective study. BMC Ophthalmol. 2019; 19 (1):180. 8.Foreman J, Salim AT, Praveen A, Fonseka D, Shu Wei Ting D, Guang He M, et al. Association between digital smart device use and myopia: a systematic review and meta-analysis. Lancet Digit Health. 2021 Dec;3(12):e806-e818. 9.Hulme C, Snowling MJ. Reading disorders and dyslexia. Curr Opin Pediatr. 2016; 28(6):731–735. 10.Brem S, Maurer U, Kronbichler M, Schurz M, Richlan F, Blau V, et al. Visual word form processing deficits driven by severity of reading impairments in children with developmental dyslexia. Sci Rep. 2020 Oct 30;10(1):18728. 11.González-Valenzuela MJ, Martín-Ruiz I. Neuropsychological Perspective on Dyslexia. In: Learning Disabilities - Neurobiology, Assessment, Clinical Features and Treatments. Intech Open; 2021. 12.Glozman J, Nemeth DG. The contributions of Luria and Reitan to developmental neuropsychology and to the understanding of neuropsychologically compromised children. In: Nemeth DG, Glozman J (Eds.) Evaluation and Treatment of Neuropsychologically Compromised Children. London: Academic Press; 2020: p. 1–26. 13.Tsybulska TE, G. Zavgorodnya NG, Pashkova OE. Predicting the risk for progression of acquired myopia in school-age children. J Ophthalmology (Ukraine). 2018;1:7-12. 14.Kobylchenko V. [Visual perception and its disorders in childhood]. Osoblyva dytyna: navchannia i vykhovannia. 2020; 4(93):46-59. Ukrainian. 15.Glozman JM, Soboleva AE. [Neuropsychological assessment of school-children]. Moscow: Smysl Publishing House; 2018. Russian. 16.Kiparenko OL. Neuropsychological determinants of dyslexia in schoolchildren. Scientific Journal of Polonia University. 2021; 46(3):235-240. 17.Luria AR. [Higher cortical functions in man]. Saint Petersburg: Piter; 2019. Russian. 18.Nielsen F. Hierarchical Clustering. In: Nielsen F (ed.). Hierarchical clustering BT - Introduction to HPC with MPI for data science. Springer; 2016;304 19.Maimon O, Rokach L. Clustering methods. In: Ed. Data Mining and Knowledge Discovery Handbook. Springer; 2006: 321–352. 20.Kiparenko O, Kremenchutska M. Assessment of the impact of motor development on adaptation to learning. Insight: the psychological dimensions of society. 2021; 6: 95-109. Disclosures Author Contribution: Kremenchutska M. K.: concept development, design, data collection, data analysis and interpretation, manuscript preparation/writing/review; Kiparenko O. L.: concept development, design, data analysis and interpretation, manuscript preparation/writing/review; Chykur L. D.: data collection and research, manuscript preparation/writing/reviewing; Pundiev V. V.: analysis and interpretation of data, preparation of the manuscript/writing; Dobrynina I. V.: manuscript preparation/writing/reviewing. All authors analyzed the results and agreed on the final version of the manuscript. Conflict of interest: The authors declare that there is no conflict of interest that could influence their opinion regarding the materials of this manuscript. Sources of support: none.
|