J.ophthalmol.(Ukraine).2021;4:39-42.
|
http://doi.org/10.31288/oftalmolzh202143942 Received: 13 June 2021; Published on-line: 16 August 2021 Accommodative convergence–accommodation ratio and fusional capacity in patients with constant and intermittent exotropia I. M. Boichuk, Alui Tarak SI "The Filatov Institute of Eye Disease and Tissue Therapy of the NAMS of Ukraine"; Odesa (Ukraine) E-mail: iryna.ods@gmail.com TO CITE THIS ARTICLE: Boichuk IM, Tarak Alui. Accommodative convergence–accommodation ratio and fusional capacity in patients with constant and intermittent exotropia. J.ophthalmol.(Ukraine). 2021;4:39-42. http://doi.org/10.31288/oftalmolzh202143942 Background: It has been reported that exotropia was seen in 16.9-23% of patients with strabismus. Exophoria and exotropia may be caused by congenital or acquired anomalies in orbital structure, ocular structure, or extraocular muscle attachment and/or location. Planning conservative treatment or time and amount of surgery for patients with exotropia will require advances in diagnostic techniques for the ocular motor and sensory system. Purpose: To determine the features of the state of accommodation and state of fusion in patients with constant and intermittent exotropia. Material and Methods: Fifty nine patients with exotropia (age, 10 to 21 years) were under surveillance. Of these, 33 (group 1) had constant exotropia and 26 (group 2), intermittent exotropia. The near point of convergence, the accommodative convergence–accommodation (AC/A) ratio and phoria and near and distance and fusion were assessed. Patients underwent a routine eye examination. In addition, the near point of convergence was determined by the proximeter, the AC/A ratio was measured by the heterophoria method, and fusional reserves were measured using the synoptophore method. Results: High AC/A ratios were more common in constant exotropia than in intermittent exotropia (53.5% versus 38%, respectively), likely due to a low accommodative convergence. The AC/A ratio was found to be statistically significantly correlated with the angle of deviation at distance in group 1 (r=0.71), angle of deviation at distance in group 2 (r=0.65), and angle of deviation at near in group 1 (r=-0.61) (p < 0.05). The interaction of accommodation and convergence was impaired since the AC/A ratio in both groups was greater than a norm value of 3-5 diopters per prism diopter. This should be taken into consideration when prescribing optical correction and orthoptic treatment for exotropia. Keywords: exotropia, accommodation, fusion, AC/A ratio
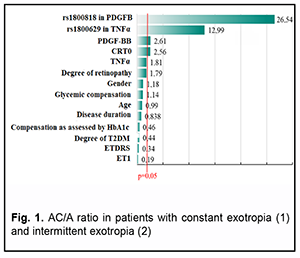
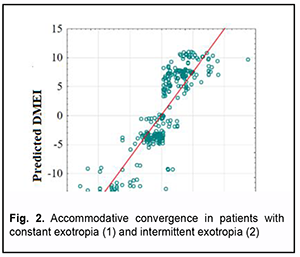
Introduction It has been reported [1] that exotropia was seen in 16.9-23%of patients with strabismus. Exophoria and exo-tropia may be caused by congenital or acquired anomalies in orbital structure, ocular structure, extraocular muscle attachment and/or extraocular muscle location [2]. The Duane’s classification is based on the difference in devia-tion for near and distance and was proposed 100 years ago. Classifications based on other factors such as state of fusion, state of convergence and primary or secondary deviation, have been proposed. The presence of apparent, intermittent or subtle deviation is controlled by fusion [3-8]. Intermittent deviation can occur in a patient with equal visual acuities, normal dextraversion and levoversion, and concomitant A or V patterns. Of note that insufficient convergence or excessive divergence does not allow to determine the cause of exotropia. The time during which the eyes are in the normal position or squint is important for clinical features of treatment of exotropia. Planning con-servative treatment or time and amount of surgery for patients with exotropia will require advances in diagnostic techniques for the ocular motor and sensory system. Although there have been isolated reports on the necessity of the assessment of the ocular vergence system, par-ticularly, the accommodative convergence–accommodation (AC/A) ratio, when prescribing conservative treatment for strabismus, the AC/A ratio in exotropia has been rather poorly investigated [1, 8, 9]. There have been isolated reports on the state of convergence, fusional capacity, and type of binocular vision in exotropia [10, 11]. Material and Methods Fifty nine patients with exotropia (age, 10 to 21 years; mean best-corrected visual acuity, 0.8 ± 0.3; mean re-fractive error, 0.95 ± 2.8) were under surveillance. Of these, 33 (group 1) had constant exotropia and 26 (group 2), intermittent exotropia. The angle of strabismus at distance and at near were 36.6 ± 2.8 and 16.6 ± 2.5 prism diop-ters, respectively, for group 1, and 30.6±2.8 and 14.0±2.3 prism diopters, respectively, for group 2, with no signifi-cant difference between groups (p > 0.05). Patients underwent a routine eye examination. In addition, the near point of convergence was determined by the proximeter, the AC/A ratio was measured by the heterophoria method (AC/A = ipd + (phoria at distance – phoria at near)/3, where ipd is the interpupillary distance in centimeters), and fusional reserves were measured using the synoptophore method. The study followed the ethical standards stated in the Declaration of Helsinki, the European Convention on Human Rights and Biomedicine and relevant laws of Ukraine. Statistica 8.0 (StatSoft, Tulsa, OK, USA) software was used for statistical analysis. Mean (M) and standard de-viations (SD) were calculated for quantitative variables. The level of significance p ≤ 0.05 was assumed. Multiple post hoc comparisons were performed using the Newman–Keuls correction or chi2 test for contingency table analy-sis. Results The mean near point of convergence was 8.8±0.9 cm for group 1 compared to 8.6±0.6 cm for group 2, but the difference was not significant (р = 0.33). There was no significant difference in the AC/A ratio between patients of group 1 and patients of group 2 (4.1 ± 2.08 diopters per prism diopter versus 3.6 ± 1.35 diopters per prism diopter, respectively, compared to a norm value of 3-5 diopters per prism diopter) (Fig. 1). In addition, the mean accommo-dative convergence was 12.4 ± 6.24 prism diopters for group 1 compared to 10.8 ± 4.05 prism diopters for group 2 (Fig. 2).
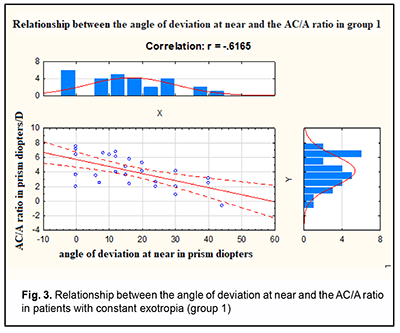
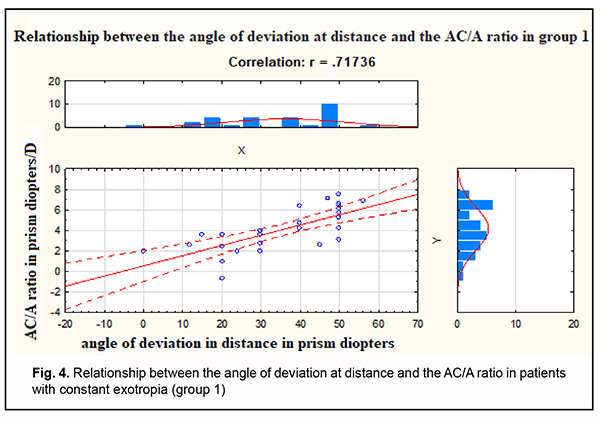
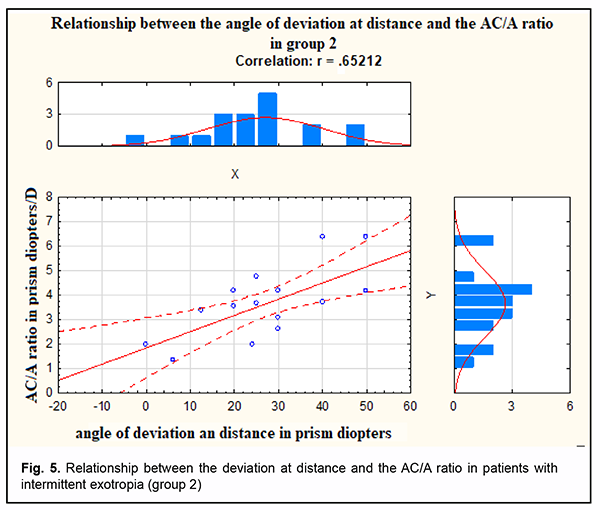
The synoptophore demonstrated a capacity for fusion significantly more frequently in patients of group 2 than in patients of group 1 (53.8% versus 24.4%; χ2 = 6.2, р = 0.001; χ2 = 4.71, р = 0.03). The correlation analysis was conducted to find out if there was an association of the AC/A ratio and visual, bin-ocular and oculomotor functions in patients with constant versus intermittent exotropia. The AC/A ratio was found to be statistically significantly correlated with the angle of deviation at distance in group 1 (r=0.71), angle of devia-tion at distance in group 2 (r=0.65), and angle of deviation at near in group 1 (r=-0.61) (p < 0.05). The data are pre-sented in Figures 3, 4, and 5.
It is well seen that the angle of deviation at distance in both groups was positively correlated with the AC/A ra-tio, whereas the angle of deviation at near in group 1 was negatively correlated. In addition, the AC/A ratio was positively significantly correlated with the angle of deviation at distance in constant exotropia (r=0.72; Fig.4) and intermittent exotropia (r=0.65; Fig. 5). However, the AC/A ratio did not correlate with visual acuity, color test data, or stereoacuity thresholds. The color test found binocular vision in 25.2% of patients of group 2, but in no patients of group 1, whereas simultaneous vision was found in 10.5% of patients of group 1. Discussion Brown [12] suggested that preoperative determination of the AC/A ratio may be helpful in predicting the extent to which a patient may respond to plus lenses when surgical overcorrection is obtained. Also, a patient with a high AC/A ratio and a basic exodeviation will manage to keep the eyes aligned when exerting normal accommodative effort at near fixation. Such a patient will respond well to minus lenses prescribed to reduce the distant deviation. Several authors [8, 9] have commented on the high incidence of high AC/A ratios in patients with exodeviations. On the other hand, von Noorden [1, 12], who determined the AC/A ratio over a range of 6D with +3.00 and -3.00 lenses in 46 patients with an apparent divergence excess, found that the AC/A ratio ranged from 3.3 to 9. We noted that high AC/A ratios were more common in constant exotropia than in intermittent exotropia (53.5% versus 38%, re-spectively), likely due to a low accommodative convergence. Fusion was observed more frequently in patients with intermittent exotropia (53.8%) than in those with constant exotropia (24.4%), χ2 = 6.2, р=0.001. On the synopto-phore, functional scotoma was demonstrated in 75.6% of patients with constant exotropia and in 46.2% of patients with intermittent exotropia. The near point of convergence was larger in group 1 than in group 2 (8.8 ± 0.9 cm ver-sus 8.6 ± 0.6), but the difference was not significant. Therefore, in exophoria with constant or intermittent strabismus, the accommodative convergence is less than a norm 15.0 prism diopters required for keeping the eyes aligned. In the current study, the interaction of accommoda-tion and convergence was impaired since the AC/A ratio was greater than a norm value of 3-5 diopters per prism diopter. This should be taken into consideration when prescribing optical correction and orthoptic treatment for exo-tropia. -+ References 1.Avetisov ES. [Concomitant strabismus]. Moscow: Meditsina; 1977. p.48-9. Russian. 2.Avetisov ES, Tarastsova MM, Khukhrina LP. [Methods and results of studies on binocular vision in preschool children]. Oftalmol Zh. 1977;32(2):86-9. Russian. 3.Kashchenko TP, Pospelov VI, Shapovalov SL. [Problems of oculomotor and binocular pathology] In: [Proceedings of the 8th Con-gress of Ophthalmologists of Russia]. Moscow, 1-4 Jun 2015. Moscow: MNTK “Eye Microsurgery” Publishing Center; 2005. p.740-1. Russian. 4.Birch EE, Gwiazda J, Held R. The development of vergence does not account for the onset of stereopsis. Perception. 1983;12(3):331-6. doi: 10.1068/p120331. 5.Burian HM. Exodeviations: their classification, diagnosis, and treatment. Am J Ophthalmol. 1966 Dec;62(6):1161-6. doi: 10.1016/0002-9394(66)92570-0. 6.Hiles DA., Davies GT, Costenbader ED. Long-term observations on unoperated intermittent exotropia. Arch Ophthalmol. 1968 Oct;80(4):436-42. doi: 10.1001/archopht.1968.00980050438006. 7.Jampolsky A. Ocular divergence mechanisms. Trans Am Ophthalmol Soc. 1970;68:730–822. 8.Jampolsky A, Flom B, Fried A. Fixation disparity in relation to heterophoria. Am J Ophthalmol. 1957 Jan;43(1):97-106. doi: 10.1016/0002-9394(57)92094-9.] 9.Noorden GK von, Brown DJ, Parks MM. Associated convergence and accommodative insufficiency. Doc Ophthalmol. 1973;34:393. 10.Noorden GK von, Campos E. Binocular Vision and Ocular motility. Theory and Management of Strabismus. Mosby: St. Louis; 2002. 11.Lee Y, Kim H. Six-month follow-up of Binocular Visual Function after Vision Therapy in Intermittent Exotropia with Three Types. J Korean Ophthalmic Opt Soc. 2020 Mar; 25(1):89-97. 12.Wu Y, Xu M, Zhang J, et al. Can Clinical Measures of Postoperative Binocular Function Predict the Long-Term Stability of Post-operative Alignment in Intermittent Exotropia? J Ophthalmol. 2020; 2020: 7392165. Conflict of Interest Statement: The authors declare no conflict of interest which could influence their opinions on the subject or the materials presented in the manuscript.
|