J.ophthalmol.(Ukraine).2020;3:42-46.
|
http://doi.org/10.31288/oftalmolzh202034246 Received: 20 February 2020; Published on-line: 24 June 2020 Prospects of up-to-date antioxidants in the treatment of chronic eye diseases O.P. Vitovska,1 L.D. Pichkur2 1Bogomolets National Medical University; Kyiv (Ukraine) 2Romodanov Neurosurgery Institute, NAMS of Ukraine; Kyiv (Ukraine) E-mail: vo.visiondep@gmail.com TO CITE THIS ARTICLE: Vitovska O.P., Pichkur L.D. Prospects of up-to-date antioxidants in the treatment of chronic eye diseases. J.ophthalmol.(Ukraine).2020;3:42-46. http://doi.org/10.31288/oftalmolzh202034246 According to the World Health Organization (WHO), about 285 million people are visually impaired, and, of those, around 39 million are blind and 246 million have low vision. About 90% of the world's visually impaired people live in low-income settings while 82% of people living with blindness are aged 50 and above; this age group represents 20% of the world's population. Age-related macular degeneration (AMD), glaucoma, cataract and diabetic retinopathy are the most common causes of legal blindness and visual impairment in Ukraine, and, today, the role of free radicals in the development of these disorders is indisputable. Astaxanthin is a powerful antioxidant, more effective than lutein or zeaxanthin. Since astaxanthin has a beneficial molecular structure and multifaceted mechanism of action, is highly bioavailable and capable of crossing the blood brain barrier, it might be promising in the treatment of chronic incapacitating disorders such as glaucoma, diabetic retinopathy and AMD. Keywords: oxidative stress, AMD, glaucoma, diabetic retinopathy, antioxidants, astaxanthin
According to the World Health Organization (WHO), about 285 million people are visually impaired, and, of those, around 39 million are blind and 246 million have low vision. About 90% of the world's visually impaired people live in low-income settings while 82% of people living with blindness are aged 50 and above; this age group represents 20% of the world's population. The global population increased by 38%, from 5.3 billion in 1990 to 7.3 billion in 2015. The world population aged and the total population over 50 years old almost doubled: from 878 million in 1990 to 1,640 million in 2015 [1]. In addition, by 2050, the global population is predicted to rise to 9.7 billion, and the number of people over the age of 60 is predicted to increase to 2.1 billion (22% of the population). The combination of a growing and an aging population will result in a massive increase in the number of people who are blind or have visual impairment due to age-related chronic diseases. The WHO, however, holds that 80 per cent of all causes of visual impairment are preventable or curable. Because the burden of chronic eye disorders is growing, the WHO coordinates global research to develop services and policy for prevention and elimination of diabetic retinopathy, glaucoma, age-related macular degeneration (AMD) and refractive abnormalities [2]. The leading global causes of blindness are cataract (65.2 million, 26%), refractive errors (123.7 million, 49%), AMD (10.4 million, 4%), glaucoma (7 million, 3%), and diabetic retinopathy (3 million, 1%) [3]. Cataract and refractive errors are common causes of curable blindness, whereas AMD, glaucoma, and diabetic retinopathy may result in irreversible loss of vision. Blindness and visual impairment are not only medical but also a social and economic problem. Previously, the International Federation on Aging predicted the global cost of vision loss to reach an alarming $2.8 trillion with indirect costs adding another $760 billion by 2020 [4]. AMD is estimated to affect more than 34 million people in the European Union. The number of patients affected by AMD in the EU is estimated to rise by almost 25% until 2050 [5]. For diabetic eye disease (DED), the current and future situation is similar. More than 25% of diabetic patients are affected by any DED, amounting to nearly 4 million individuals in the EU. Each year, 4.6% of Europeans with diabetes are newly affected by any DED, corresponding to more 770,000 individuals in the EU per year. Given the increasing global prevalence of diabetes, the number of patients with diabetic retinopathy is expected to rise dramatically. Thus, the number of EU inhabitants affected by any DED has been estimated to increase by 6% by 2040 [5]. The most common ocular disorders in adults in Ukraine are myopia, cataract, glaucoma and conjunctival disorders. In 2014, conjunctival disorders (including conjunctivitis), cataract, myopia, and retinal disorders accounted for 12.63%, 15.6%, 12.44%, 7.41%, and 0.6% of the total eye disease in this country. In addition, in 2015, glaucoma was the most common cause of legal blindness and visual impairment, followed by retinal disorders and ocular trauma. Therefore, although the prevalence of these disorders is relatively low, they are the leading causes of blindness in this country and present a major medical and social problem [6, 7, 8]. Though it is generally acknowledged that there is a relationship between aging and AMD, the pathogenesis of the disease is not completely understood. AMD is a multi-factorial disorder with multiple predisposing factors, including age, heredity, metabolic and hemorheologic disorders, and oxidative stress, with the latter playing an important role. Cells require oxygen to generate energy and produce free radicals as by-products of chemical reactions with oxygen. When there are too many free radicals, they can set off a damaging chain reaction, which in turn can result in cell death, particularly in nerve cells. Oxidative stress is manifested by activation of free radical oxidation and oxidative injury to proteins, DNA and membrane lipids. On the other hand, oxidative stress is an imbalance between pro-oxidants and antioxidants (or between oxidation and reduction). In other words, oxidative stress results when there is increased production of free radicals or decreased activity of antioxidants. The factors contributing to the formation of free radicals are called pro-oxidative factors. Of these, the most important for the development of ocular disease are exposure to short-wave radiation, smoking, presence of harmful chemical substances in the environment, etc. Today, the role of free radicals in the development of such disorders as AMD, glaucoma, cataract and diabetic retinopathy is undisputable. Antioxidants, a key component of the antioxidant system, are the substances that are capable of counteracting the damaging effect of free radical oxidation. These include vitamins, enzymes, proteins, etc. In addition, they can be divided into two categories: enzymatic and non-enzymatic [9, 10, 11]. The latter include minerals (copper, selenium, zinc, etc.); vitamins B, A, E, and C; carotenoids (?-carotene, lutein, canthaxanthin, zeaxanthin, astaxanthin etc.). Carotenoids comprise a family encompassing more than 600 pigments. They are thought to be important for retinal health and prevention of retinal disorders. The retina is constantly affected by light and oxygen, the factors that induce the formation of free radicals. In addition, the retina is vulnerable to oxidative stress and hypoxia. Antioxidative properties of carotenoids are responsible for their photo-, radio-, and cancer-protective effects [12]. Some researchers believe that carotenoids exert their antioxidative effects in two ways. First, they are found in maximum levels in the macula, and are located in the pigment epithelium, and, in this way, may exert direct antioxidative effects. Second, they act as a filter protecting the retina from light damage. Astaxanthin, a red pigment found in marine life (salmon, trout and shrimps) and some birds (e.g., quail), is a powerful antioxidant, more effective than lutein or zeaxanthin. The green algae Haematococcus pluvialis, the red yeast, and Phaffia rhodozyma are common sources of natural astaxanthin. Unusual chemical properties of astaxanthin and its bioavailability are explained by its molecular structure [13]. Astaxanthin has two carbonyl groups, two hydroxyl groups, and eleven conjugated ethylenic double bonds. Astaxanthin may act as a strong antioxidant by donating the electrons and reacting with free radicals to convert them to more stable product and terminate free radical chain reaction in a wide variety of living organisms [14, 15]. In general, polar carotenoids (e.g. free astaxanthin) tend to be of higher bioavailability than apolar species (e.g. beta-carotene) [16]. In recent years, a number of studies on astaxanthin have in vitro and in vivo demonstrated its antioxidant effect [17, 18]. It was reported that astaxanthin could inhibit lipid peroxide formation and enhance the antioxidant enzyme status [19]. Exposure of lipids and tissues to light, especially UV-light, can lead to production of singlet oxygen species and subsequently and photo-oxidative damage of these lipids and tissues. Astaxanthin can be significantly more effective than beta-carotene and lutein at preventing UV-light photooxidation of lipids [20, 21]. In some cases, astaxanthin has up to several-fold stronger free radical antioxidant activity than vitamin E and b-carotene. It has been generalized that astaxanthin has an antioxidant activity, as high as ten times more than other carotenoids such as zeaxanthin, lutein, canthaxantin, and beta-carotene, and 100 times more than tocopherol, and thus has been dubbed a ‘‘super vitamin E’’ [22]. Astaxanthin has also been reported to exert other effects, such as protection against cancer, inflammation, and diabetes, immunomodulatory and neuroprotective effects [23]. Unlike beta-carotene, astaxanthin never becomes a pro-oxidant. Animal studies demonstrated that astaxanthin is capable of crossing the blood brain barrier and, similar to lutein, will deposit in the retina of mammals. Nagaki et al. [24] found that 6mg of astaxanthin per day could improve eye fatigue in visual display terminal workers. According to an oxidative stress development theory, impaired circulation results in a shortage of or no antioxidants entering the problematic area. Given this, it is important that astaxanthin might increase retinal capillary blood flow in both eyes in normal volunteers and intraocular pressures remained unchanged during the supplementation period [25]. In addition, Izumi-Nagai et al. [26] concluded that astaxanthin treatment significantly suppressed the development of choroidal neovascularization. Free radicals have been found to be involved in cataract formation and associated with damage to lens protein structure and subsequent lens opacification. Astaxanthin was found to be capable of providing appreciable protection for beta high-crystallin against oxidative stress, and thus capable of preventing the development of cataract [27]. Liao et al. [25] reported that astaxanthin could interact with selenite, whose accumulation in the lens might cause cataract formation directly. Nakajima et al. [28] found that astaxanthin had neuroprotective effects against retinal ganglion cell damage. Cort et al. [29] showed that astaxanthin significantly decreased the percent of apoptotic cells on the retina in rats with elevated intraocular pressure. This study confirmed the role of oxidative injury in elevated intraocular pressure and highlighted the protective effect of astaxanthin in ocular hypertension [29]. Otton et al. [30, 31] showed that astaxanthin could be a good adjuvant in prophylaxis or recovery of lymphocyte dysfunctions associated with diabetic patients. In addition, Hussein et al. [32] investigated the effects of astaxanthin in a metabolic syndrome animal model and found that astaxanthin significantly lowered the levels of blood glucose and triglycerides, and significantly increased the levels of high-density lipoprotein cholesterol. The authors, therefore, concluded that astaxanthin ameliorates insulin resistance and improves insulin sensitivity. Chan et al. [33] showed that astaxanthin enhanced cell and mitochondrial membrane stability. These studies suggested that astaxanthin had the protective effects on a neurodegenerative disease, and might be a promising neuroprotective therapeutic agent for oxidative stress-associated neurodegeneration such as Parkinson’s disease [33, 34]. Therefore, since astaxanthin has a beneficial molecular structure and multifaceted mechanism of action, is highly bioavailable and capable of crossing the blood brain barrier, it might be promising in the treatment of chronic incapacitating disorders such as glaucoma, diabetic retinopathy and AMD. 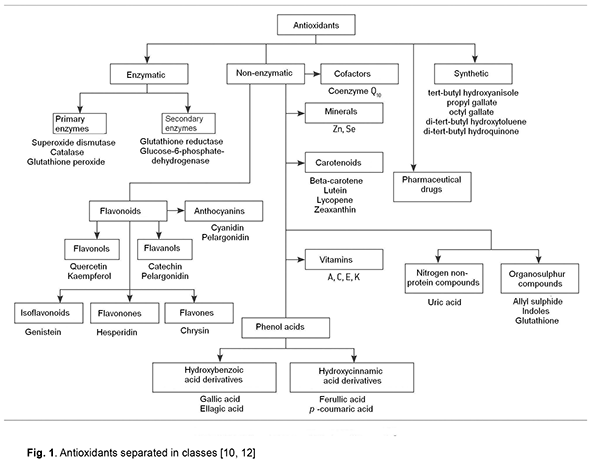
References 1.Ackland P, Resnikoff S, Bourne R. World blindness and visual impairment: despite many successes, the problem is growing. World blindness and visual impairment: despite many successes, the problem is growing. Community Eye Health. 2017;30(100):71–3. 2.World Health Organization. Blindness and Vision Impairment. [(accessed on 14 June 2019)];Available online: https://www.who.int/news-room/fact-sheets/detail/blindness-and-visual-im.... 3.Vitovska OP. [Health promotion strategy in ophthalmology]. Russkii meditsinckii zhurnal. Klinicheskaia odtalmologiia. Glaukoma. 2013;3:88–92. Russian. 4.Chader GJ, Taylor A. Preface: The Aging Eye: Normal Changes, Age-Related Diseases, and Sight-Saving Approaches. Invest Ophthalmol Vis Sci. 2013 Dec 13;54(14):ORSF1-4. 5.Li JQ, Welchowski T, Schmid M. Retinal diseases in Europe: prevalence, incidence and healthcare needs. European Society of Retina Specialists (EURETINA). 2017; 1–28. Available online: http://www.euretina.org/downloads/EURETINA_Retinal_Diseases.pdf 6.Vitovska OP, Vasiuta VA. [Pathways for improving medical care for patients with optic nerve atrophy]. Skhidnoievropeiskyi zhurnal gromadskogo zdorovia. 2015;1(26):58–9. Ukrainian. 7.Vitovska OP, Alifanova TA, Poveshchenko IuL. [Epidemiological aspects of primary disability caused by glaucoma in Ukraine]. Oftalmologiia. 2016;2(4):16–26. Russian. 8.Vitovska OP, Vasiuta VA. [Analysis of the dynamics of prevalence of optic nerve atrophy in Ukraine]. Visnyk naukovykh doslidzhen. 2015;3:72–5. Ukrainian. 9.Polumbryk M, Ivanov S, Polumbryk O. Antioxidants in food systems. Mechanism of action. Ukr J Food Sci. 2013;1:15—40. 10.Carocho M, Ferreira I.C.F.R. A review on antioxidants, prooxidants and related controversy: natural and synthetic compounds, screening and analysis methodologies and future perspectives. Food Chem Toxicol. 2013 Jan;51:15-25. 11.Reznikov AG, Polumbryk OM, Balion IaG, Polumbryk MO. [Pro- and anti-oxidative systems and pathological processes in the human body]. Visnyk NAN Ukrainy. 2014;10:17-29. Ukrainian. 12.Britton G. [The Biochemistry of Natural Pigments]. Moscow: Mir; 1986. Russian. 13.Kishimoto Y, Tani M, Uto-Kondo H, Iizuka M et al. Astaxanthin suppresses scavenger receptor expression and matrix metalloproteinase activity in macrophages. Eur J Nutr. 2010; 49: 119–26. 14.Hussein G, Goto, H, Oda, S, Sankawa, U et al. Antihypertensive potential and mechanism of action of astaxanthin: III. Antioxidant and histopathological effects in spontaneously hypertensive rats. Biol Pharm Bull. 2006; 29:684–8. 15.Ranga Rao A, Raghunath Reddy RL, Baskaran V, Sarada R, Ravishankar GA. Characterization of microalgal carotenoids by mass spectrometry and their bioavailability and antioxidant properties elucidated in rat model. J Agric Food Chem. 2010 Aug 11;58(15):8553-9. 16.Bohn T. Bioavailability of non-provitamin A carotenoids. Curr Nutr Food Sci. 2008;4:240–58. 17.Miki W. Biological functions and activities of animal carotenoids. Pure Appl Chem. 1991;63:141–6. 18.Palozza P, Krinsky NI. Astaxanthin and canthaxanthin are potent antioxidants in a membrane model. Arch Biochem Biophys. 1992 Sep;297(2):291-5. 19.Nishigaki I, Rajendran P, Venugopal R, Ekambaram G et al. Cytoprotective role of astaxanthin against glycated protein/iron chelate-induced toxicity in human umbilical vein endothelial cells. Phytother Res. 2010 Jan;24(1):54-9. 20.Papas AM. Antioxidant Status, Diet, Nutrition, and Health. Washington, DC: CRC Press; 1999. 21.Greene L. Asthma and oxidant stress: Nutritional, environmental, and genetic risk factors. J Am Coll Nutr. 1995 Aug;14(4):317-24. Crossref PubMed 22.Higuera-Ciapara I, F?lix-Valenzuela L, Goycoolea FM. Astaxanthin: a review of its chemistry and applications. Crit Rev Food Sci Nutr. 2006; 46(2):185–96. Crossref PubMed 23.Hussein G, Sankawa U, Goto H, Matsumoto K, Watanabe H. Astaxanthin, a carotenoid with potential in human health and nutrition. J Nat Prod. 2006 Mar;69(3):443-9.Crossref PubMed 24.Nagaki Y, Mihara M, Tsukahara H, Ono S. The supplementation effect of astaxanthin on accommodation and asthenopia. J Clin Ther Med. 2006; 22:41–54. 25.Liao JH, Chen CS, Maher TJ, Liu CY et al. Astaxanthin interacts with selenite and attenuates selenite-induced cataractogenesis. Chem Res Toxicol. 2009 Mar 16;22(3):518-25.Crossref PubMed 26.Izumi-Nagai K, Nagai N, Ohgami K, Satofuka S, Ozawa Y, Tsubora K et al. Inhibition of choroidal neovascularization with an anti-inflammatory carotenoid astaxanthin. Invest Ophthalmol Vis Sci. 2008 Apr;49(4):1679-85. 27.Wu TH, Liao JH, Hou WC, Huang FY, Maher TJ, Hu CC. Astaxanthin protects against oxidative stress and calcium-induced porcine lens protein degradation. J Agric Food Chem. 2006 Mar 22;54(6):2418-23. 28.Nakajima Y, Inokuchi Y, Shimazawa M, Otsubo K, Ishibashi T, Hara H. Astaxanthin, a dietary carotenoid, protects retinal cells against oxidative stress in vitro and in mice in vivo. J Pharm Pharmacol. 2008 Oct;60(10):1365-74. 29.Cort A, Ozturk N, Akpinar D, Unal M, Yucel G, Ciftcioglu A, et al. Suppressive effect of astaxanthin on retinal injury induced by elevated intraocular pressure. Regul Toxicol Pharmacol. 2010 Oct;58(1):121-30. 30.Otton R, Marin DP, Bolin AP, Santos RDe C, Polotow TG, Sampaio SC, et al. Astaxanthin ameliorates the redox imbalance in lymphocytes of experimental diabetic rats. Chem Biol Interact. 2010 Aug 5;186(3):306-15. 31.Nishigaki I, Rajendran P, Venugopal R, Ekambaram G, Sakthisekaran D, Nishigaki Y. Cytoprotective role of astaxanthin against glycated protein/iron chelate-induced toxicity in human umbilical vein endothelial cells. Phytother Res. 2010 Jan;24(1):54-9. 32.Hussein G, Nakagawa T, Goto H, Shimada Y, Matsumoto K, Sankawa U, et al. Astaxanthin ameliorates features of metabolic syndrome in SHR/NDmcr-cp. Life Sci. 2007 Jan 16;80(6):522-9. 33.Chan KC, Mong MC, Yin AC. Antioxidative and anti-inflammatory neuroprotective effects of astaxanthin and canthaxanthin in nerve growth factor differentiated PC12 cells. J Food Sci. 2009 Sep;74(7):H225-31. 34.Liu XB, Shibata T, Hisaka S, Osawa T. Astaxanthin inhibits reactive oxygen species-mediated cellular toxicity in dopaminergic SH-SY5Y cells via mitochondria-targeted protective mechanism. Brain Res. 2009 Feb 13;1254:18-27.
The paper was supported by 'Valartin Pharma'
|