J.ophthalmol.(Ukraine).2020;2:79-86.
|
http://doi.org/10.31288/oftalmolzh202027986 Received: 15 January 2020; Published on-line: 30 April 2020
Developing the inter-role conflict scale for eye-care workers N.V. Rodina 1, Dr Sc (Psychology),Prof.; B.V. Biron,1 Cand Sc (Psychology); A.I. Ukhanova, 1 Cand Sc (Psychology); N.S. Semeniuk,2 Cand Sc (Psychology); A.V. Kernas,3 Cand Sc (Psychology) 1 Mechnikov National University of Odesa; Odesa (Ukraine) 2 IQVIA RDS Ukraine; Odesa (Ukraine) 3 Ukrainian Communication Academy Science and Technical Centre, Department of Natural Science and Psychological Harmonization of Personality Development; Odesa (Ukraine) E-mail: nvrodinaod@gmail.com TO CITE THIS ARTICLE: Rodina NV, Biron BV, Ukhanova AI, Semeniuk NS, Kernas AV. Developing the inter-role conflict scale for eye-care workers. J.ophthalmol.(Ukraine).2020;2:79-86. http://doi.org/10.31288/oftalmolzh202027986
Background: Eye care workers are highly prone to the risk of psychological problems due to emotional demands of job and high stress loads. Because inter-role conflicts act as stress load factor, it is important to develop psychometrically adapted psychodiagnostic instruments for detecting them. Purpose: To develop a Ukrainian version of the psychometric scale as a tool for measuring inter-role conflicts for eye care workers, to psychometrically analyze it, and to estimate its relationships with stress reactions. Material and Methods: The study sample consisted of the eye care workers from the Filatov institute. Two hundred and eleven eye care workers were requested to respond to relevant questions. The response rate was 85.8% (181/211). The 181 responders included 99 nursing staff members and 82 ophthalmologists. The adapted version of the 1996 Netemeyer’s et al Work-Family Conflict and Family-Work Conflict Scales and the Stress Reaction Inventory for eye care workers designed by Ukrainian researchers, Tsekhmister, Daniliuk, Rodina, Biron, and Semeniuk, were used in the study. Results: The Inter-role Conflict Scale was developed by adapting the Netemeyer’s et al questionnaire. The modified version of the scale is comprised of the two subscales describing two forms of inter-role conflicts, Work-Family Conflict (WFC) and Family-Work Conflict (FWC); these subscales were found to have high internal consistency and test-retest reliability. The two-factor scale model was verified by a confirmatory factor analysis. The two forms of inter-role conflicts were found to be statistically more severe in the physician staff than in the nursing staff. The test norms were developed and presented using the quartile scale, as long as the sample was representative. Therefore, the adapted Ukrainian-language version of the Inter-role Conflict Scale for eye care workers showed evidence of internal consistency and construct validity. Keywords: inter-role conflict, stress, psychometric scale, ophthalmologists
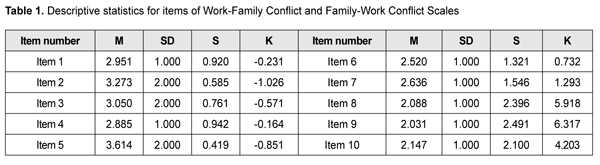
Introduction Role conflicts as a social and psychological phenomenon are of great importance for the worker’s activity. Among other organizational factors, inter-role conflict acts as a mediator of the interrelationship between the worker’s ability to perform the work and his/her actual performance of the work [1]. A role conflict is an attribute of certain professions, and a number of studies have been published on conflicts that arise for doctors (physicians [2], oncologists [3], surgeons [4], etc.) and other medical care workers between work and family roles. To the best of our knowledge, only few studies (to be exact, one Canadian study [5] and two Indian studies [6, 7]) have been published on inter-role conflicts for eye care workers, which makes this study important. Therefore, the purpose of this paper was to develop and psychometrically analyze a Ukrainian version of the psychometric scale designed specifically to assess inter-role conflicts for medical care workers and examine these conflicts in their relationships with stress reactions. Material and Methods The study sample consisted of the eye care workers from the Filatov institute and ophthalmology departments of South Ukraine hospitals. Two hundred and eleven eye care workers were requested to respond to relevant questions. The response rate was 85.8% (181/211). The 181 responders included 99 nursing staff members, and 82 ophthalmologists. The Work-Family Conflict and Family-Work Conflict Scales designed by American researchers, Netemeyer, Boles, and McMurrian [8], were used to study the balance between work and personal life in these workers. The results of translation of these scales and their psychometric adaptation to the Ukrainian population were described in this paper. The methodology comprised of two subscales. The first subscale consisted of 5 items and described the situations in which demands from the work domain impeded family domain performance. The second subscale also consisted of 5 items and described the situations in which demands from the family domain impeded work domain performance. The responders check a box for the items using a 7-point Likert-type scale from 1 (strongly disagree) to 7 (strongly agree). A decentered translation [9] of the relevant items from English to Ukrainian was made, aiming at both loyalty of meaning and equal familiarity and colloquialness in both languages in the questionnaire text, and taking into account the social and cultural norms. The translated version was named the Inter-role Conflict Scale for eye care workers. The Stress Reaction Inventory (SRI) for eye care workers designed by Ukrainian researchers, Tsekhmister, Daniliuk, Rodina, Biron, and Semeniuk [10] showed evidence of internal consistency and construct validity, and was used to analyze the criterion validity of the methodology subjected to psychometric adaptation. In this inventory, the four categories representing Reactions to Stressors are Physiological (F), Emotional (G), Behavioral (H), and Cognitive Appraisal (I). Results In the first stage of the study, the psychometric analysis of the Inter-role Conflict Scale for eye care workers was conducted. Each item of the scale receives a direct score. The descriptive statistics for scale items are given in Table 1.
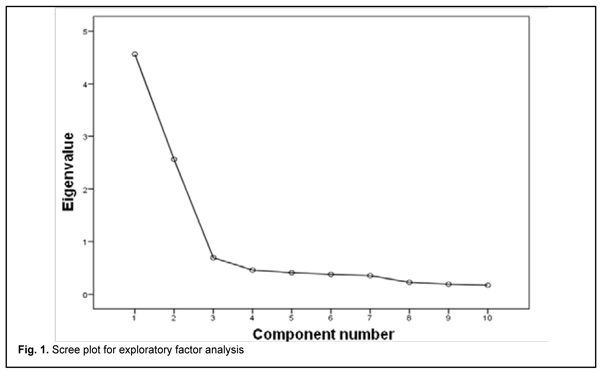
All items were normally distributed (Table 1). According to Kline [11], if the asymmetry value is less or equal to 3, and the excess value is less or equal to 10, the normality of the distribution is acceptable. In addition, rigorous multidimensional normality test such as Mardia’s multivariate kurtosis was conducted [12]; Mardia’s multivariate kurtosis coefficient was 79.436, which was significantly less than a critical value of 120. Therefore, the maximum likelihood modeling method could be used for confirmatory factor analysis. The exploratory factor analysis included all 10 items and was used to determine the number of factors in the model. The factor analysis was conducted using the maximum likelihood method. Bartlett’s test of sphericity (test of at least one significant correlation between 2 of the items studied) was used to evaluate the “factorability” of our data and was significant (?2 = 1146.567, p < .001). The Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy was 0.835, above the commonly recommended value. The number of factors required for an adequate factor solution was determined using the scree plot (Fig. 1).
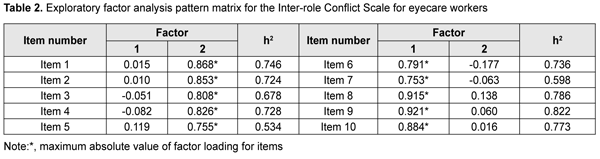
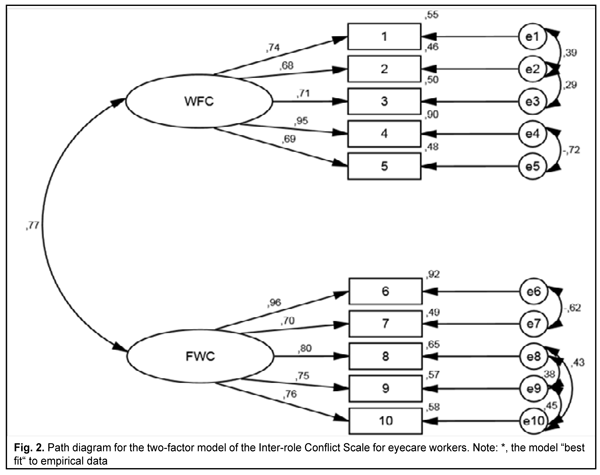
Based on this plot, a two-factor model seemed to be appropriate, and we decided to examine and modify this model. This model explains 71.233% of the total variance in initial variables. Therefore, a substantial portion of data contained in the questionnaire would be maintained, with the first factor explaining 45.606%, and the second factor, 25.626% of the total variance in initial variables. Promax oblique rotation was selected to produce both factor pattern and factor structure matrices. Table 2 presents the pattern matrix resulting from the exploratory factor analysis for the Inter-role Conflict Scale for eye care workers. The first factor included all the items reflecting the work-family conflict, whereas the second factor comprised the items reflecting the family-work conflict (Table 2). The two-factor model comprising a complete set of items was subjected to confirmatory factor analysis, which did not prove a good initial fit to the data (Table 2, Model 1). This made us to modify the initially obtained two-factor model. The regression coefficients for the effects of latent variables on the observed variables (items) were found to be high (? > 0.600; p < 0.01), which allowed to retain all the items in the model. The modification indices indicated that it was necessary to consider correlations between residual variances of the following items: 1 and 2, 2 and 3, 4 and 5, 6 and 7, 8 and 9, 8 and 10, 9 and 10.
Figure 2 presents the finally modified two-factor model. The model fit indices calculated for the modified two-factor model (Table 3, Model 2) indicated that the model complied requirements on almost all cut-off norms. Thus, chi-square per-degree-of-freedom (?2/df) ratios of less than 3 indicate good fit [11]. A Standardized Root-Mean-Square Residual (SRMR) less than 0.08 indicate a well-fitting model [13]. The Root-Mean-Square Error of Approximation (RMSEA) values may give rise questions with regard to the goodness of fit. RMSEA fit index is an estimate of the discrepancy between the model and the data per degree of freedom for the model. It has been suggested that values less than 0.05 constitute good fit, values in the 0.05 to 0.08 range acceptable fit, and values in the 0.08 to 0.10 range marginal fit [14].
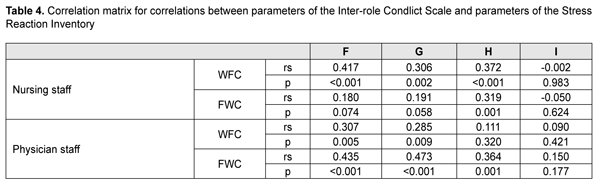
In addition, Normed-Fit Index (NFІ), Incremental Fit index (ІFI) and Comparative Fit Index (CFI) were used; compared to the above fit indices, they are less affected by sample size and number of degrees of freedom. For the goodness of fit, NFI and CFI values [15] as well as IFI values [16] should be equal to or higher than 0.90. Therefore, the two-factor structure allowed us to develop the two subscales, with the first comprising items numbered 1 to 5 and describing the work-family conflict, and the second comprising items numbered 6 to 10 and describing the family-work conflict. Cronbach's Alpha test [17] was conducted to test internal reliability, and McDonald’s omega (?B) [18] was computed as an additional estimate of internal reliability. The internal reliability was found to be high since the relevant values were higher than norms (Cronbach's alpha > 0.60 and ?B > 0.60) [19]. This was true with regard to both the work-family conflict subscale (alpha = 0.907, ?В = 0.876), and the family-work conflict subscale (alpha = 0.880, ?В = 0.837). Because the intersubscale correlation coefficient was strong (r = 0.770; p < 0.001), we tested the hypothesis that the one-factor model is consistent with the empirical data. The one-factor model comprising all items from the scales was subjected to confirmatory factor analysis, which did not provide a good fit to the empirical data (Table 3, Model 3). Although the modification (Table 3, Model 3) of the obtained one-factor model allowed improving substantially the initial version of the model, the modified one-factor model was worse fit than Model 2 which was accepted as the basis for developing the Inter-role Conflict Scale for eye care workers. We, however, find it promising to conduct further research on developing a one-factor Ukrainian-language questionnaire based on the Inter-role Conflict Scale for eye care workers. The internal reliability for the whole scale comprising 10 items was also found to be high (Cronbach's alpha =0.916 and ?B = 0.823). While considering psychological content of either subscale separately, it should be noted that the first subscale (the work-family conflict (WFC) subscale) characterizes the role conflict in which the general demands of, time devoted to, and strain created by the job interfere with performing family-related responsibilities. The family-work conflict (FWC) subscale characterizes the intensity of inter-role conflict in which the general demands of, time devoted to, and strain created by the family interfere with performing work-related responsibilities. The Pearson correlation coefficient was calculated after retest and indicated that two-week test-retest reliability was high. Thus, Pearson coefficients for the WFC subscale and FWC subscale were 0.793 and 0.851, respectively, among the nursing staff, and 0.838 and 0.799, respectively, among the physician staff. Therefore, the subscales of the Inter-role Conflict Scale (IRCS) are characterized also by high test-retest reliability for empirical research. The last stage of the psychometric analysis for this methodology consisted in examination of the descriptive statistics for constructed scales. Descriptive statistics for the WFC and FWC subscales were (M = 2.973; SD = 0.976) and (M = 2. 177; SD = 0.875), respectively, among the nursing staff subsample, and (M = 3.374; SD = 0.978) and (M = 2.415; SD = 0.662), respectively, among the physician staff subsample. A comparison among contrast groups with regard to intensity of inter-role conflicts was performed using the Mann-Whitney U test. The test found significant differences with regard to the WFC subscale (U = 3325.500; p = 0.035) and the FWC subscale (U = 3145.500; p = 0.005). Therefore, the intensity of inter-role conflicts depended on the eye care worker’s official capacity, and was higher among the ophthalmologist staff than among the nursing staff. In addition, the intensity of the WFC was higher than the intensity of the FWC among both the former and the latter staff. Thus, one may conclude that, among eye care workers, demands from the work domain impede family domain performance more than demands from the family domain impede work domain performance. Criterion-related validity was assessed by Spearman’s correlation between the Inter-role Conflict Scale (IRCS) and the Stress Reaction Inventory (Table 4).
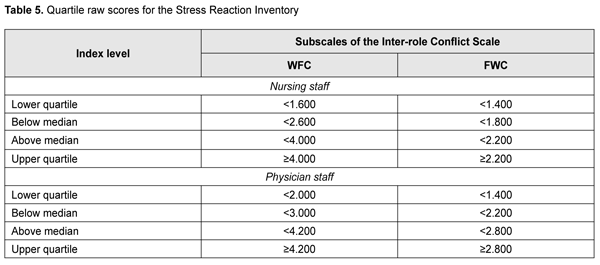
The table demonstrates that, among the nursing staff, the presence of WFC is reflected in reactions to physiological and behavioral stressors, burnout, etc., whereas FWC is reflected only in reactions to behavioral stressors. In addition, among the ophthalmologist staff, the presence of the WFC is reflected in reactions to physiological and emotional stressors, whereas the FWC is reflected in reactions to physiological, emotional and behavioral stressors, etc. The last stage of the study was to standardize the Inter-role Conflict Scale. We believe that the study sample can be used to standardize the questionnaire, and that the norms calculated for the sample are representative for the individuals of relevant age and social status. This makes it possible to introduce relevant test norms. The method selected for reducing normalized estimates to the easy-to-use form boils down to presenting final test estimates using a quartile scale (Quartile 1, lower quartile; Quartile 2, below median; Quartile 3, above median; Quartile 4, upper quartile). The table shows raw index scores corresponding to defined standardized index levels in accordance with calculated quartile estimates. Thus, taking into consideration that the sample is representative of the target population, were developed the test norms expressed in quartiles.
Discussion It has been reported that ophthalmologists are at high risk of psychological distress due to high demands on professional activity [5]. Because ophthalmologists have reported high levels of burnout [20] and work stress [21] associated primarily with their responsibility to the patient [22], ophthalmology is a particularly suitable subject for studying the factors associated with professional distress. The present study focuses on assessing inter-role conflicts for Ukrainian eye care workers. While conceptualizing the inter-role conflict as a stress factor, it should be noted that no psychodiagnodtic tool for assessing work-family and family-work role interference for medical professionals has been published yet in Ukrainian. These conflicts in the works of Ukrainian researchers have been studied only in general terms, as “the work-life balance of personnel”, using the methodology developed by Tkalych [23]. In this connection, we developed and psychometrically analyzed the Ukrainian version of the Work-Family Conflict and Family-Work Conflict Scales, the version that was named the Inter-role Conflict Scale and designed for eye care workers. In addition, we estimated the relationships of this psychodiagnostic tool with stress reaction indices. Comparison of the two subscales in scores for responders demonstrated that, for most responders, the family was more valuable than work. The authors of the Work-Family Conflict and Family-Work Conflict Scales have predicted previously [24] that the WFC scale has a higher mean score than the FWC scale, which was also characteristic for our study sample. In general, the level of WFC and FWC among eye care workers was lower than guideline values obtained for the English-language sample and Russian-language sample with the English version [8] and adapted Russian version [24], respectively, of the Work-Family Conflict and Family-Work Conflict Scales. This indicates that representatives of the study sample do not tend to consider that work and family impede critically each other. These inter-role conflicts were more severe in the physician staff than in the nursing staff due to higher pressure, and, consequently, higher interference of role responsibilities. Our estimation of relationships between the parameters of the IRCS and the Stress Reaction Inventory (SRI) for eye care workers draws us to the following conclusions. The role conflict is known to be an important factor of work-related stress (the role stressor or work-schedule-related stressor category) [1]. Long exposure to role conflict leads to various destructive (cognitive, emotional and behavioral) consequences for personality. Cognitive consequences include decreased self-assessment, self-image discrepancy, recognition of having a personal problem in choice of values to which (s)he should commit himself/herself, and doubt of the truth of motives and principles. Emotional consequences include psychoemotional strain, apparent negative feelings, a decrease in satisfaction with activities, and negative emotional background of communication. Behavioral consequences include decreased quality and intensity of performance and absenteeism [25]. Organizational consequences of WFC have been described generally as low labor satisfaction, staff burnout, turnover intention or leaving the organization, and decreased performance, whereas family consequences of WFC have been described generally as depression, general family dissatisfaction and general life dissatisfaction [8]. The absence of significant correlation with cognitive stress appraisal shows that reflection of inter-role conflict-induced stress is not associated with conflict intensity. This indicates irrationality of the perceived load of stressful events and stress coping efficacy under conditions of inter-role conflict. Application of the standardized IRCS would allow comparing the results of further studies with those of the current study. In practical terms, the scale can be widely used in test batteries for assessing the efficacy of psychological support for the eye care staff. A study by Nair and colleagues [6] concluded that good family support and an understanding partner help ophthalmologists achieve good work-life balance. The current study is limited by not taking into accounts certain important parameters such as gender, professional experience, number of children in the family, and other social and demographic variables. The questionnaire is provided in the Appendix.
References 1.Weiner IB, Borman WC, Ilgen DR, Klimoski RJ (Eds.). Handbook of psychology. V. 12. Industrial and organizational psychology. NJ, Hoboken: John Wiley & Sons, Inc; 2003. 2.Fuss I, N?bling M, Hasselhorn HM, Schwappach D, Rieger MA. Working conditions and Work-Family Conflict in German hospital physicians: psychosocial and organisational predictors and consequences. BMC Public Health. 2008 Oct 7;8:353. 3.Kleiner S, Wallace JE. Oncologist burnout and compassion fatigue: investigating time pressure at work as a predictor and the mediating role of work-family conflict. BMC Health Serv Res. 2017; 17: 639. 4.Dyrbye LN, Shanafelt TD, Balch CM, Satele D, Sloan J, Freischlag J. Relationship between work-home conflicts and burnout among American surgeons: a comparison by sex. Arch Surg. 2011; 146(2):211-7. 5.Viviers S, Lachance L, Maranda MF, M?nard C. Burnout, psychological distress, and overwork: The case of Quebec's ophthalmologists. Canadian J Ophthalmol. 2008 Oct;43(5):535-46. 6.Nair AG, Jain P, Agarwal A, Jain V. Work satisfaction, burnout and gender-based inequalities among ophthalmologists in India: A survey. Work. 2017;56(2):221-8. 7.Saurabh K, Sarkar K, Roy R, Majumder PD. Personal and practice profile of male and female ophthalmologists in India. Indian J Ophthalmol. 2015 Jun;63(6):482-6. 8.Netemeyer RG, Boles JS, McMurrian R. Development and Validation of Work-Family Conflict and Family-Work Conflict Scales. J Appl Psychol. 1996;81(4):400–10. 9.Campbell D. [Models of experiments in social psychology and applied researches]. St. Petersburg: Socialno-psikhologicheskii tsentr. 1996. Russian. 10.Tsekhmister IV, Daniliuk IV, Rodina NV, Biron BV, Semeniuk NS. Developing a stress reaction inventory for eye care workers. Journal of Ophthalmology (Ukraine). 2019;1(486):39-45. 11.Kline RB. Principles and Practice of Structural Equation Modeling. New York: The Guilford Press; 2005. 12.Mardia KV. Measures of multivariate skewness and kurtosis with applications. Biometrika. 1970:57, 519–30. 13.Hu LT, Bentler PM. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria Versus New Alternatives. Structural Equation Modeling. 1999; 6(1):1-55. 14.Fabrigar LR, MacCallum RC, Wegener DT, Strahan EJ. Evaluating the use of exploratory factor analysis in psychological research. Psychological Methods. 1999;4(3):272–99. 15.Bentler PM, Bonett DG. Significance tests and goodness of fit in the analysis of covariance structures. Psychological Bulletin. 1980;88(3):588-606. 16.Bollen K. A New Incremental Fit Index for General Structural Equation Models. 1989;17(3):303–16. 17.Cronbach LJ. Coefficient alpha and the internal structure of tests. Psychometrika. 1951;16:297–334. 18.McDonald RP. Test theory: A unified treatment. Mahwah, NJ: Erlbaum; 1999. 19.Hair JF, Black WC, Babin BJ, Anderson RE. Multivariate Data Analysis. Prentice Hall: Upper Saddle River, New Jersey; 2010. 20.Medscape Ophthalmologist Lifestyle Report 2018: Personal Happiness vs. Work Burnout. [Last accessed on 2018 Mar 20]. Available from: https://www.medscape.com/slideshow/2018-lifestyle-ophthalmologist-6009233#1. 21.Ulrich LR, Lemke D, Erler A, Dahlhaus A. [Subjective and objective work stress among ophthalmologists in private practice in Thuringia : Results of a state-wide survey]. Ophthalmologe. 2019 Jul;116(7):647-655. DOI: 10.1007/s00347-018-0802-1. German. 22.Stewart WC, Stewart JA, Adams MP, Nelson LA. Survey of practice-related stress among United States and European ophthalmologists. Graefes Arch Clin Exp Ophthalmol. 2011 Sep;249(9):1277-80. 23.23. Tkalych MG. [The"work-life" balanceofpersonnel:the substantiationofempirical indicators]. Problemy suchasnoi psychologii. 2017;(1):85-90. Ukrainian. 24.Smirnova AIu. [The impact of role conflict on job insecurity]. Organizatsionnaia psikhologiia. 2016;6(4):14-29. Russian. 25.Berezovskaia TA. [The level of role conflict as an index of manager’s professional health]. In: Schelkova OIu (Ed.). [Proceedings of the Ananiev Memorial Lectures: Psychology in Public Health]. 2013 May 22-24; St. Petersburg, Russia. p. 419-20. Russian. APPENDIX Instruction Please provide the number of the response choice (1 = strongly disagree, 2 = disagree, 3 = neither agree nor disagree, 4 = agree, 5 = strongly agree) that reflects your degree of agreement with statements below. 1. The demands of my work interfere with my home and family life. 2. The amount of time my job takes up makes it difficult to fulfill family responsibilities. 3. Things I want to do at home do not get done because of the demands my job puts on me. 4. My job produces strain that makes it difficult to fulfill family duties. 5. Due to work-related duties, I have to make changes to my plans for family activities. 6. The demands of my family or spouse/partner interfere with work-related activities. 7. I have to put off doing things at work because of demands on my time at home. 8. Things I want to do at work don't get done because of the demands of my family or spouse/partner. 9. My home life interferes with my responsibilities at work such as getting to work on time, accomplishing daily tasks, and working overtime. 10. Family-related strain interferes with my ability to perform job-related duties. Survey results processing: Below are the numbers of items incorporated in the scales. Subjects respond to the inventory by rating each item using a seven-point scale. The raw score is computed as the mean of responses for all items in an individual scale. The Family Work Scale (FWC) comprises items nos. 1, 2, 3, 4, and 5. The raw score is divided by 5. The Work Family Scale (WFC) comprises items nos. 6, 7, 8 , 9 and 10. The raw score is divided by 5. The data are compared with those in the table of quartile rawscores for the Stress Reaction Inventory (Table 5). The authors certify that they have no conflicts of interest in the subject matter or materials discussed in this manuscript.
|