J.ophthalmol.(Ukraine).2018;2:61-66.
|
http://doi.org/10.31288/oftalmolzh201926166 Received: 05 February 2019; Published-online: 24 April 2019 Case Report: Solar retinopathy following exposure to reflected sunlight A.S. Krivoruchko, Ophthalmologist; K.G. Drachenko, Senior Research Fellow; S.K. Drachenko, technician; A.R. Korol, Dr Sc (Med) Filatov Institute of Eye Disease and Tissue Therapy; Odesa (Ukraine) E-mail: anastasiakrivoruchko2593@gmail.com TO CITE THIS ARTICLE: Krivoruchko AS, Drachenko KG, Drachenko SK, Korol AR. Case Report: Solar retinopathy following exposure to reflected sunlight. J.ophthalmol.(Ukraine).2019;2:61-6. http://doi.org/10.31288/oftalmolzh201926166 Background: Radiation damage to the eye is most commonly caused by sunlight. Solar retinopathy is a form of retinal damage that occurs after exposure to solar radiation, with the most common symptoms being reduced vision and central scotoma. Purpose: To report a case of retinal damage following exposure to reflected sunlight with a favorable outcome. Materials and Methods: The patient underwent visual acuity, tonometry, ophthalmoscopy, optical coherence tomography (OCT), fundus photography and fluorescein angiography. Results: At six months after initiation of treatment, the patient reported that the white spot before his left eye decreased in size, and became transparent and practically unnoticeable to him. In solar retinopathy, the OCT appearance of retinal defect may vary, depending on the severity of damage, but provides evidence of destruction of the outer retinal layers. Conclusion: We reported a case of retinal damage following exposure to reflected sunlight with a favorable outcome. Follow-up OCT showed complete restoration of the affected retinal structures in one eye and the residual changes in the outer photoreceptor layer and RPE in the fellow eye. Therefore, solar retinopathy can occur with OCT evidence of retinal destruction following retinal damage from direct and/or reflected sunlight. Keywords: retina, photoreceptors, pigment epithelium, solar retinopathy, reflected sunlight
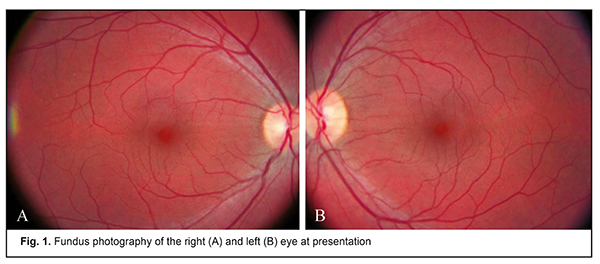
Introduction Radiation damage to the eye is most commonly caused by sunlight. Ultraviolet keratitis [1, 2] and solar retinopathy [3-6] are attributed to sunlight-induced ocular damage. The Sun is a natural source of light and produces electromagnetic radiation across a wide range of wavelengths, from radio waves to X-rays. Visible sunlight can get to the retina and cause pathological changes in retinal structures, which may lead to impaired visual function [7]. Solar retinopathy (damage to the retina from solar radiation) is a clinical entity specifically recognized in the International Classification of Diseases (ICD) version 10 nomenclatures [3-6]. Although the name of the disease includes the word “retina”, it is, rather, the macula that is affected in this disorder. Our lids act as the first barrier protecting the eye from a sudden, intensive illumination. UV-A and visible sunlight can get to the retina and cause pathological changes in retinal structures, which may lead to impaired visual function [7]. Another protective mechanism is a reflexive response to light (iris contraction) [8]. In addition, protective antioxidative pigments such as the kynurenines, located in the human lens, and melanin, in the uvea and retina, absorb ambient radiation and dissipate its energy without causing damage [5]. The macular pigments (lutein, zeaxanthin and meso-zeaxanthin) absorb light (with maximum absorption taking place at ~460 nm) are estimated to absorb 40% to 90% of incident blue light, and therefore, function as an intraocular filter and play an important role in fundus protection against visible shortwave radiation [9]. The melanin within the RPE cells absorbs light that has not been captured by the photoreceptors, thus preventing excessive light scattering within the eye and enhancing visual system resolution [8, 9]. Retinal damage severity depends upon the transparency of the ocular media. Young individuals are mostly affected since their ocular media are relatively transparent to radiation [10, 11]. Histopathological studies have demonstrated that it is the RPE and retinal photoreceptor outer segments that are most susceptible to sunlight-induced damage [3, 12]. The purpose was to report a case of retinal damage following exposure to reflected sunlight with a favorable outcome. Materials and Methods A 31-year-old man presented to the Laser Microsurgery Department of the Institute with complaints of visual discomfort and a 2-3-mm white fixed spot before his left eye 3 days after he came back from his trip to the USA where he had spent much time watching Mojave Desert car races without eye protection under bright sunlight conditions. He reported that while watching the races he had been not looking at the sun directly, but had a feeling of visual discomfort from bright sunlight reflected off sand and car windscreens. The patient believed that this could lead to the subsequent visual discomfort and the spot before his left eye. He had not any history of previous visual complaints, and his previous visual acuity test results were rather high. The patient underwent visual acuity, tonometry, ophthalmoscopy, optical coherence tomography (OCT; first visit, Optopol Spectral Domain OCT Copernicus+; second and third visits, Optopol Spectral Domain OCT REVO NX), fundus photography and fluorescein angiography (Topcon TRC-50IX Fundus Camera). He received antioxidant treatment in the form of parabulbar injections of methyl ethyl pyridine hydrochloride, anti-inflammatory treatment (parabulbar injections of dexamethasone phosphate), retinal protective treatment (intramuscular injections of morpholinium salt of tiazotic acid), and nutritional vitamin supplement. Results At presentation, visual acuity was 2.0 both OD and OS, and IOP measured with a Maklakoff tonometer was 19 mmHg both OD and OS. The initial objective findings in the right eye were as follows: no pathologic changes in the anterior eye; the ocular media were clear; the optic disc was pale pink, physiologically excavated, and with clear margins; the foveal reflex was dull; and there was no peripheral retinal pathology. The initial objective findings in the left eye were as follows: no pathologic changes in the anterior eye; the ocular media were clear; the optic disc was pale pink, physiologically excavated, with clear margins; the foveal reflex was dull and appeared somewhat widened as compared to the right eye; and no pathologic changes in the peripheral retina (Fig. 1).
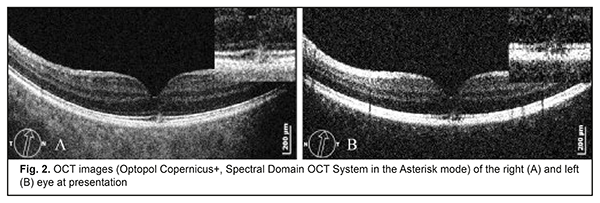
In addition, OCT showed deformation of the retinal profile at the foveola in the form of swelling of the retinal photoreceptor inner and outer segments without damage to the RPE in the right eye, and deformation of the retinal profile at the foveola in the form of swelling of the retinal photoreceptor inner and outer segments with partial RPE damage in the left eye (Fig. 2).
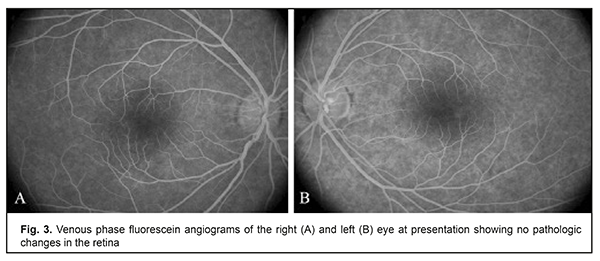
No pathological changes in the retina of either eye were observed during any phase of the angiogram (Fig. 3).
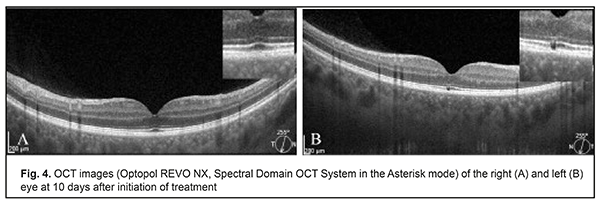
A diagnosis of bilateral solar retinopathy (H31.0 as per the ICD-10 criteria) was made based on examination findings. At 10 days after initiation of treatment, visual acuity was 2.0 both OD and OS. In addition, the objective findings in the right eye were as follows: no pathologic changes in the anterior eye; the ocular media were clear; the optic disc was pale pink, physiologically excavated, and with clear margins; the foveal reflex was distinct; and no peripheral retinal pathology. The objective findings in the left eye were as follows: no pathologic changes in the anterior eye; the ocular media were clear; the optic disc was pale pink, physiologically excavated, with clear margins; the foveal reflex was dull; and no pathologic changes in the peripheral retina. Moreover, in the right eye, OCT showed no pathologic changes in the retinal profile of the inner and outer retinal layers. In the left eye, OCT demonstrated deformation of the retinal profile in the form of window defect in the projection of both the retinal photoreceptor outer segments and RPE at the foveola, and no pathologic changes in the retinal profile of the inner retinal layers (Fig. 4).
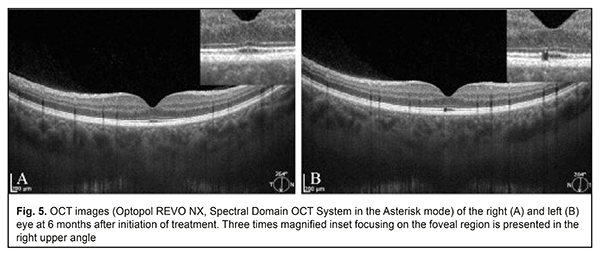
At six months after initiation of treatment, the patient reported that the white spot before his left eye decreased in size, and became transparent and practically unnoticeable to him. Visual acuity was 2.0 both OD and OS. In addition, objective findings in both eyes did not change from the previous visit. Moreover, OCT showed no changes from scans at 10 days (Fig. 5).
The residual changes in the outer photoreceptor layer and RPE in the left eye were consistent with the complaint of visual defect in this eye. Discussion Sunlight does not cause direct thermal damage, but can induce photochemical damage to the retina. Solar retinopathy develops mainly through photooxidation [13]. The mechanism involves changes in photoreceptor membranes and alterations in RPE function due to excess solar radiation absorption by melanin [6, 14]. The RPE maintains the integrity of photoreceptor inner-segment/outer-segment junction, and executes phagocytosis of photoreceptor outer segments [8]. RPE cell dysfunction results in death of retinal photoreceptors and neurons, and, consequently, leads to loss of visual function [15]. In 2000, Bechmann et al [6] were the first to report OCT images showing retinal structural changes in solar retinopathy. They revealed a hyporeflective area at the fovea and all overlying retinal layers were affected. In our case, the defect was located in the projection of both the retinal photoreceptor outer segments and RPE. In the case reported by Chen and Lee [16], at 3 months after presentation with solar retinopathy, cross-sectional retinal images produced by the OCT revealed localized loss of RPE cells at the centre of the fovea, with normal overlying retinal layers. The authors, however, did not report on the features of the retinal photoreceptor layer. Ibragimova and Bilandarli [7] reported a case of solar maculopathy in 2010. In that case, OCT findings included a hyporeflective foveal region at the level of hyporeflective photoreceptor outer segment layer and partially hyporeflective RPE layer at presentation, and normal reflectivity of all retinal layers at 5 months. In our case, however, OCT images demonstrated that the foveal defect did not change in size or shape even at month 6 compared to day 10. Another case of solar maculopathy has been presented in the atlas by Aznabaev et al [17]. The OCT scans crossing the central fovea displayed a dot-shaped destruction of the IS/OS and photoreceptor outer segment layer with insubstantial deformation of adjacent retinal layers caused by detritus, which is close to our findings [17]. Pomytkina et al [18] reported a case of unintended retinal damage from reflected sunlight. In that case, a driver presented with complaints of abrupt loss of vision and a spot in his central vision in his left eye after accidentally looking at the sun ray reflected at the side-view mirror. In addition, left eye OCT images demonstrated (a) highly or moderately reflective foci in the projection of the outer and inner retinal layers (which evidenced disorganization of these layers), (b) defects of a highly reflective band formed by the signal reflected from the photoreceptor inner-segment/outer-segment junction, and (c) a highly reflective RPE-choriocapillaris complex with its internal contour scalloped because of the presence of thinned locations. In the current case, the patient also reported visual discomfort from the reflected sunlight, but did not experience a decrease in visual acuity. The retinal OCT changes in the case reported by Pomytkina et al [18], however, were more apparent than in the case reported here. Therefore, in solar retinopathy, the OCT appearance of retinal defect may vary, depending on the severity of damage, but provides evidence of destruction of the outer retinal layers. Conclusion We reported a case of retinal damage following exposure to reflected sunlight with a favorable outcome. Follow-up OCT showed complete restoration of the affected retinal structures in one eye and the residual changes in the outer photoreceptor layer and RPE in the fellow eye. Therefore, solar retinopathy can occur with OCT evidence of retinal destruction following retinal damage from direct and/or reflected sunlight. References 1.Schein OD. Phototoxicity and the cornea. J Natl Med Assoc. 1992 Jul;84(7):579–83. 2.Guly HR. Snow Blindness and Other Eye Problems During the Heroic Age of Antarctic Exploration. Wilderness Environ Med. 2012 Mar;23(1):77–82. 3.Hope-Ross MW, Mahon GJ, Gardiner TA, et al. Ultrastructural findings in solar retinopathy. Eye (Lond). 1993;7 (Pt 1):29–33. 4.Gurko TS. [Analysis for patients with photic retinal damage following viewing of an eclipse]. Vestnik Orenburgskogo gosudarstvennogo universiteta. 2015;12:187. Russian. 5.Akhmetshin RF, Abdulaeva EA, Bulgar SN. [Solar maculopathy. Results of five years of follow-up]. Kazanskii meditsinskii zhurnal. 2013;94(6):901–3. Russian. 6.Bechmann M, Ehrt O, Thiel MJ, et al. Optical coherence tomography findings in early solar retinopathy. Br J Ophthalmol. 2000;84:547–8. 7.Ibragimova NM, Bilandarli LSh. [Solar maculopathy and diagnostic value of OCT. Case report]. Oftalmologiya. 2010;2:80–2. Russian. 8.Vit VV. [The structure of the human visual system]. Odessa: Astroprint; 2003. p.664. 9.Pasyechnikova NV, Naumenko VA, Korol AR, Zadorozhnyy OS. [Infrared diagnostics in ophthalmology]. Odesa: TES; 2014. Russian. 10.Boettner EA, Wolter JR.Transmission of the ocular media. Invest Ophthalmol. 1962;1:776–83. 11.Pasyechnikova N, Naumenko V, Korol A, Zadorozhnyy O. Digital imaging of the fundus with long-wave illumination. Klin oczna. 2009;111(1-3):18–20. 12.Tso MO, La Piana FG. The human fovea after sungazing. Trans Sect Ophthalmol Am Acad Ophthalmol Otolaryngol. 1975 Nov-Dec;79(6):OP788–95. 13.Glickman RD. Ultraviolet phototoxicity to the retina. Eye Contact Lens. 2011 Jul;37(4):196–205. 14.Michaelides M, Rajendram R, Marshall J, Keightley S. Eclipse retinopathy. Eye. 2001 Apr;15(Pt 2):148–51. 15.Likhvantseva VG, Ziangirova GG, Fedorenko AV, et al. [Investigating the efficacy of retinal repair through transplantation of cultured RPE (experimental study)]. Ufa: Vostok Zapad; 2011. p.245–-7. Russian. 16.Chen JC, Lee LR. Solar retinopathy and associated optical coherence tomography findings. Clin Exp Optom. 2004 Nov;87(6):390–3. 17.Aznabaev BM, Mukhamadeev TR, Dibaev TI. [Optical coherence tomography + angiography of the eye]. Moscow: August Borg; 2015. Russian. 18.Pomytkina NV, Zhirov AL, Sorokin TL. [Atypical case of solar retinopathy]. Vestn Oftalmol. 2017;133(2):99-103.
The authors certify that they have no conflicts of interest in the subject matter or materials discussed in this manuscript.
|