J.ophthalmol.(Ukraine).2017;6:20-24.
|
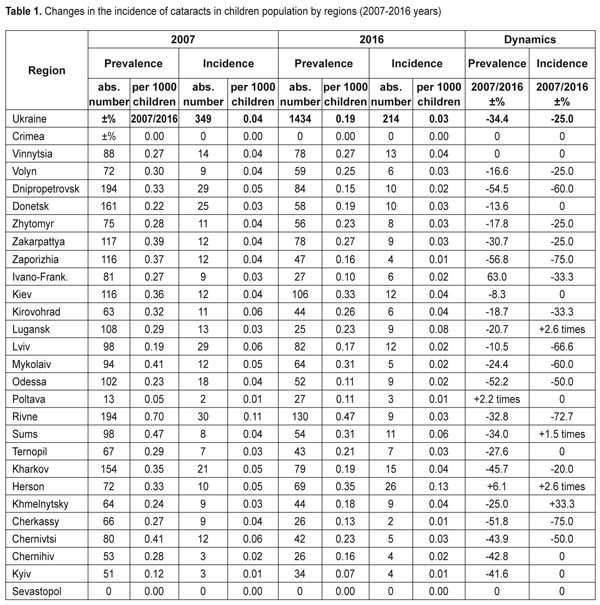
https://doi.org/10.31288/oftalmolzh201762024 The level of pediatric cataract in regions according to data of Ministry of Health of Ukraine for 2007-2016 years M. O. Chornobai, Cand. Sc. (Med.) Ophthalmic Genetics and Visual Function Branch, National Eye Institute, National Institutes of Health Bethesda, MD (USA) E-mail: chornobai.mariia@nih.gov The purpose of this study was to examine the changes in incidence and prevalence of cataract during the 10-year period between 2007-2016 among children who had been registered in the Health Care of Ukraine. In Ukraine, the cataract prevalence was among children above the average as compared to other countries in Europe. The cataract prevalence decreased in most regions (except Poltava region where it increased 2.2 times and Kherson region where in increased by 6.1%). The worst situation of pediatric cataract incidence was in Rivne region, the best one was in Poltava region. Over 10 years, the cataract incidence did not change in seven regions and increased in Sumy and Kherson regions. The cataract incidence decreased by 75% in Cherkasy and Zaporizhia regions. Dynamic of pediatric cataract showed the worst situation in the Kherson region and the best one in Zaporizhia region. Over the period 2007-2016, there was a decrease in prevalence and incidence of cataract in all age groups of children. The cataract incidence in rural population of children prevailed over children in the urban area, especially it was noticeable in 2015. There was a positive dynamics, especially in the cataract prevalence in children from the urban area. The incidence of cataract in adolescent girls was less than in boys, but there was a positive dynamics regarding the cataract prevalence among the teenagers, except the cataract incidence in boys which did not change. The cataract incidence increased with age, the highest level were recorded in the adult population (18 and older). Among the children population, the incidence reached the highest rates in adolescence. Keywords: pediatric cataract, prevalence, incidence Introduction Childhood blindness in Ukraine is on the third place in the overall structure of child disability. [1] A good understanding of risk factors is essential for the development of successful prevention programs. This is a priority for the program "Prevention of blindness and visual impairment" - a global program to eliminate blindness by 2020. [14] According to statistics in 2012, in Ukraine there are 8,553 children with poor vision and legally blind, of which 715 are blind in both eyes. [4] Among the 10,000 Ukrainian children population 1 child is blind [4] . A disease is hereditary in approximately 50% of children with congenital pathology. The average frequency of congenital and hereditary diseases is 40-60 per 1,000 births. [2] Cataract represents a substantial part of disability of children worldwide and is diagnosed in one or both eyes early on, starting from birth (congenital), in childhood or adolescence. [9] With the incidence of 1-3 cases per 10,000 live births, congenital / infantile cataract is a rare but threatening condition for vision. [7] Late diagnosis and intervention of this curable disease can lead to blindness due to amblyopia. [10] Etiological studies of pediatric cataract have estimated that genetic causes account for 10–39% of pediatric cataract/cases. However, this may be an underestimate since approximately 50–60% of cases are deemed idiopathic. [5, 11, 13] Early and continuous identification of children with eye pathology, and therefore family’s carriers of hereditary eye disease, modern medical rehabilitation of children with hereditary pathology of the eye, and most importantly, measures of prevention of birth of children with hereditary pathology of the eye is one of the main tasks of ophthalmogenetics. [3] The purpose of this study is to examine the changes in incidence and prevalence of cataract during the 10-year period between 2007-2016 among children who were registered in the health care of Ukraine. The study of the epidemiology of pediatric patients with cataracts can provide the basis for strategies that will be used to develop prevention and treatment of this disease that causes childhood blindness. Materials and Methods Statistical data records of the Ministry of Health of Ukraine (Form 12, "The structure and incidence of diseases by classes and individual etiological forms") during 2007-2016 were used as baseline data to calculate the frequency of cataracts in children and adolescents registered in child health-care institutions of Ukraine. Total considered 2,496 cases of cataracts in children aged 0-17 in 2007; 1793 cases in 2013; 1,669 cases in 2014; 1,500 cases in 2015; 1,434 cases in 2016. In statistical report for the 2014-2016, patients were divided into 3 groups according to age as follows: 0-6 years, 7-14 years, 15-17 years. Data on patients in 2007 and 2013 were divided into 2 groups: 0-14 years old, 15-17 years old. Clinical classification of cataract was not presented and, consequently, correlation of phenotype to genotype was impossible in those cases. In the future, cases should be classified according to their congenital and hereditary defects for individualized treatment and prevention tactics. The results of DNA studies may be a more effective basis for the classification of cataracts than clinical data. Statistical analysis All data were entered into Microsoft Excel (Microsoft Corp., Redmond, WA, USA) spreadsheets, absolute frequency (n) and relative frequency (%) were used for qualitative variables such as prevalence and incidence of cataracts. Results and Discussion As it is shown in Table 1, in 2007 cataract is most common among children in Rivne region - 0.7 per 1,000 children, Sumy region - 0.47 per 1,000 children, Mykolaiv and Chernivtsi regions - 0.41 per 1,000 children; in 2016: in Rivne region - 0.47 per 1,000 children, Kherson - 0.35 per 1,000 children, and Kyiv regions 0.33 per 1,000 children. The least common cataract in 2007 was in Poltava region- 0.05 per 1,000 children and Lviv region - 0.19 per 1,000 children; in 2016: in the Ivano-Frankivsk, Odesa and Poltava - 0.1 per 1,000 children. So, the worst situation regarding prevalence is in Rivne region, the best one is in Poltava region.
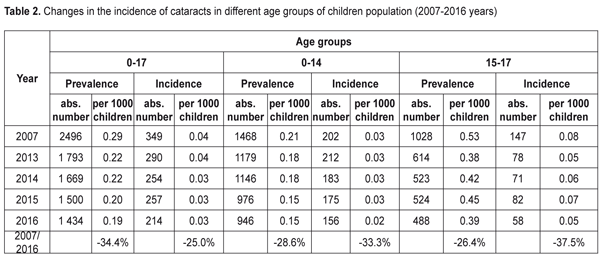
For incidence, the highest rating in 2007 was in Rivne, Kirovograd, Lviv and Chernivtsi regions; in 2016 – in Kherson and Sumy (except for Luhansk and Donetsk regions, which were not considered). The lowest detected cataracts in children were in Poltava and Chernihiv regions in 2007 and in Poltava and Zaporizhia regions in 2016. Thus, in general, the worst situation of incidence of pediatric cataract was in Rivne region and the best one in Poltava. The highest incidence was in 2016 in Kherson region, which was 0.13 per 1,000 children. Regarding the prevalence of cataract, in most regions it was decreasing (except in the Poltava region where it increased 2.2 times and Kherson region where it increased by 6.1%). The prevalence decreased by 56.8% in the Zaporizhia region, by 54.5% in Dnipropetrovsk region while only by 8.3% in Kyiv region and by 10.5%.in Lviv. Over 10 years the incidence did not change in seven regions and even increased in Sumy and Kherson. The incidence decreased by 75% in Cherkasy and Zaporizhia regions. Thus, regarding the dynamics, generally, the worst situation was in the Kherson region, the best one was in Zaporizhia region. As it is shown in Table 2, for the 2007-2016 in all age groups there was a decrease in incidence of cataract; generally, in group of 0-17 years old the prevalence and incidence of cataracts decreased by 34.4% and by 25.0%, respectively. Most of the decrease in incidence was in 15-17 aged adolescents and 0-14 aged children: by 37.5% and 33.3%, respectively.
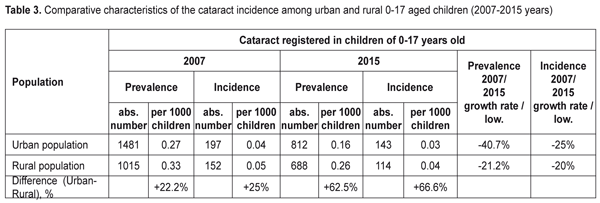
The prevalence and incidence of cataract in adolescents of 15-17 years old dominated 2.5 times above those in children of 0-14 years old and this trend continued during the last decade. According to Rahi J.S. and Dezateux C. etiological distribution of pediatric cataract in UK is divided as follows: idiopathic bilateral, 37%, and one-sided, 92%; inherited bilateral, 56%, and unilateral, 6%; due to systemic disorders and infections bilateral 6%, and unilateral, 2%. [14] Registration of congenital and inherited cataract anomalies divided into etiological distribution groups will improve the prevention and treatment of this eye disease and can be used to develop methods for molecular diagnostics in affected families. As it is shown in Table 3, the cataract incidence prevails in rural children over children in the urban area, especially it is noticeable in 2015. However, there is a positive dynamic, especially in the cataract prevalence and the positive dynamics is more expressed in urban children.
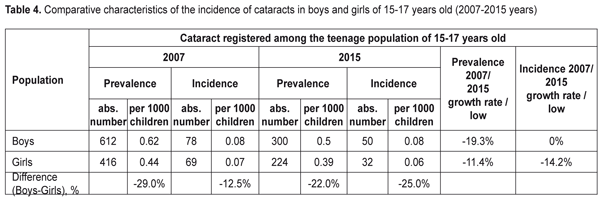
As it is shown in Table 4, the incidence of cataracts in adolescent girls was less than in adolescent boys, but there is a positive dynamics regarding the prevalence of cataracts of the teenagers except incidence in the boys which did not change.
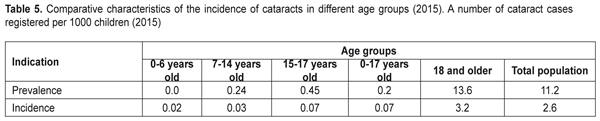
In terms of areas, the higher cataract prevalence was obserbed in teen age boys in Rivne (1.24 per 1,000) and Kyiv (1.08) regions and in teen age girls in Vinnitsa (1.03) and Sumi (0.91) regions. The lowest rate of cataract incidence were in boys and girls in Odessa region,0.33 and 0.19 per 1,000 children, respectively. Whereas, cataract prevalence rates among children in European countries are 2.49-3.46 per 10,000 children in the UK; 4.0 per 10,000 children in Sweden; 2.3 per 10,000 in Denmark [13]. We can make a conclusion that in Ukraine the cataract prevalence level is above the average, compared to other countries in Europe. The highest incidence of primary cataract occurs in boys in Zaporizhia (0.18 per 1000) and Kyiv (0.17) regions and in girls in Dnipropetrovsk (0.18) and Sumi (0.21) regions. In some regions of Ukraine there were no cataract cases newly-onset in teenagers in 2015. In 2007, there was a different ratio for the regions, except Rivne region which had the highest cataract among teenagers. As it is shown in Table 5, the cataract incidence increased with age, the highest levels were recorded in the adult population (18 and older). Among the children, the cataract incidence reached the highest rates in adolescants.
Conclusions 1. In Ukraine, the cataract prevalence among children is above the average as compared to other countries in Europe. The prevalence of cataract in most regions decreased (except Poltava region where it increased 2.2 times and Kherson region where it increased by 6.1%). The worst situation of the pediatric cataract incidence was in Rivne region, the best one was in Poltava region. Over 10 years, the incidence did not change in seven regions and increased in Sumy and Kherson regions. The cataract incidence decreased by 75% in Cherkasy and Zaporizhia regions. Dynamic of pediatric cataract showed the worst situation in Kherson region and the best one in Zaporizhia region. 2. For the period of 2007-2016, there was a decrease in prevalence and incidence of cataract in all age groups of children. 3. The incidence of cataracts in rural children prevailed over children in the urban area, especially it was noticeable in 2015. There was a positive dynamics, especially in the cataract prevalence in children from the urban area. 4. The cataract incidence in adolescent girls was less than in adolescent boys, but there was a positive dynamics regarding the cataract prevalence in teenagers, except the incidence in boys which did not change. 5. The incidence of cataract increased with age, the highest levels were recorded in the adult population (18 and older). Among the childre population, the cataract incidence reached the highest rates in adolescence. References
|