J.ophthalmol.(Ukraine).2017;2:8-11.
|
https://doi.org/10.31288/oftalmolzh20172811 Relationship between diabetic retinopathy and cognitive impairment in patients with type 2 diabetes mellitus
Zherdiova N.N., Cand. Sc. (Med.) Medvedovskaya N.V., Dr. Sc. (Med.) Mankovsky B.N., NAMS corr.-member, Prof., Dr. Sc. (Med.) Shupik National Medical Academy of Postgraduate Education Kyiv, Ukraine E-mail: zherdeva@bk.ru
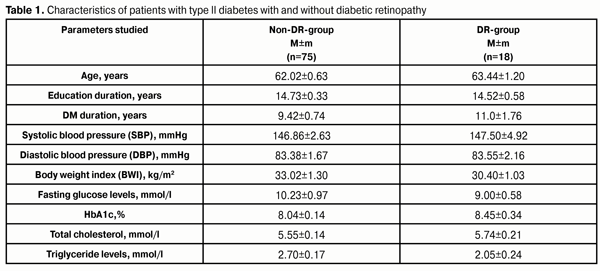
Background. Retinal microcirculation disorders can be diagnosed at the early stage of complication development while cerebral circulation disorders and cognitive impairment are diagnosed at a rather late stage, when structural changes develop in the brain of the patients. Most authors have investigated the cognitive function by studying memory, information and operation processing speed not taking into consideration the sensitivity of tests in this group of patients. The relationship between diabetic retinopathy and cognitive impairments has not investigated. The purpose of the present study was to investigate the state of cognitive function in type 2 diabetes patients with diabetic retinopathy and to determine the most sensitive cognitive tests. Material and Methods. The study included 93 patients with type 2 diabetes, aged 50 to 80. The patients were divided into two groups: DR-group and non-DR group. Cognitive function was studied using tests as follow: a “five words” test, Mini-mental State Examination (MMSE); Frontal Assessment Battery (FAB), a clock drawing test, a “fifteen words” test, the Brixton test, the Trail making test (TMT), Digit span forward and backforward (DSFB), the Verbal fluency test, the Тest symbol and the Stroop color test. Results. The TMT test showed significantly better performance in regard of working memory, memory flexibility, and executive functions in the group of patients without DR as compared to those with retinopathy. Statistically significant impairment of the executive function in patients with DR was confirmed by the Brixton test in comparison with that parameter in non-DR-group. According to the TMT and the Brixton test, patients without DR had better performance of working memory and memory flexibility as well as executive functioning compared to DR patients, which indicates lesions of frontal and prefrontal areas of the brain in those patients with DR. The Brixton test seems to be more sensitive and easy to use for screening the cognitive impairments in patients with diabetes mellitus and DR. Key words: diabetes mellitus, mild cognitive impairment, dementia, diabetic retinopathy Background Diabetes Mellitus is a metabolic disease leading to such complications as neuropathy, retinopathy, and nephropathy. According to the UK Prospective Diabetes Study (UKPDS) data, micro vascular complications are revealed when diabetes is diagnosed, which is associated with late diagnosis of the disease [1]. Also, diabetes is associated with an increased risk of dementia especially in groups where mild cognitive impairments have been diagnosed [2, 3]. But, unfortunately, though retinal microcirculation disorders can be diagnosed at the early stage, cerebral circulation disorders with cognitive impairment development are diagnosed at a rather late stage when structural changes develop in the brain of the patients. Recent researches on association between cognitive impairment (CI) and diabetic retinopathy (DR) have received conflicting data [4, 5]. The presence of DR has been shown to increase a risk of mild cognitive impairment (MCI) development more than twice (OR 2.36) [6]. A systematic review, including six studies, has also determined the increase in cognitive impairment risk (OR -2.0) in type 2 diabetes patients with DR [7]. Another study has found the association between DR and MCI only in male subjects [8]. Also, cognitive dysfunction has been more apparent in patients with mild DR signs than in a group of severe DR [9]. Furthermore, the most authors have investigated the cognitive function by studying memory, information and operation processing speed not taking into consideration the sensitivity of tests in this group of patients. The purpose of the present study was to investigate the state of cognitive function in type 2 diabetes patients with DR and to determine the most sensitive cognitive tests. Material and Methods The study included 93 patients with type 2 diabetes, aged 50 to 80. The patients were divided into two groups: DR-group and non-DR group. Exclusion criteria were the presence of another diabetes type, alcohol abuse, craniocerebral trauma, a history of insult, professional diseases that could affect the study, and depressive disorders. In order to reveal the depressive disorders, we used two questionnaires: • Centre for Epidemiologic Studies Depression Scale (CES-D) • Hospital Anxiety and Depression (HAD) A patient was excluded from the study if he/she had 19 CES-D scores and 11 and more HAD scores, which meant the presence of depression. Cognitive function was studied using tests as follow: a “five words” test, Mini-mental State Examination (MMSE); Frontal Assessment Battery (FAB), a clock drawing test, a “fifteen words” test, the Brixton test, the Trail making test (TMT), Digit span forward and backforward (DSFB), the Verbal fluency test, the Тest symbol and the Stroop color test. Ophthalmological examination included: oblique illumination examination to assess the eyelids, tear organs, conjunctiva; visual acuity test; tonometry using a non-contact portative transpalpebral tonometer to measure IOP; biomicroscopy of the anterior eye; direct and indirect ophthalmoscopy with preliminary phenylephrine mydriasis to examine the eye fundus. Changes in the eye fundus in DR were assessed according to classification as follows: 1) Nonproliferative diabetic retinopathy 2) Preproliferative diabetic retinopathy 3) Prolifirative diabetic retinopathy Patients with stage II-III DR were included in DR group. Statistical data processing was performed using SPSS version 23.0 for Windows. A general linear model (UNIANOVA), adjusted for age, educational level, and gender, was used to compare DR-group and non-DR-group. T-test was also used to compare the data between groups. The difference between parameters was considered significant with р<0.05. Results and Discussion The patients had no statistically significant difference between groups in regard to age, education level, and disease duration. Characteristics of patients are given in Table 1. The data are given as Mean value ± error of mean (М±m).
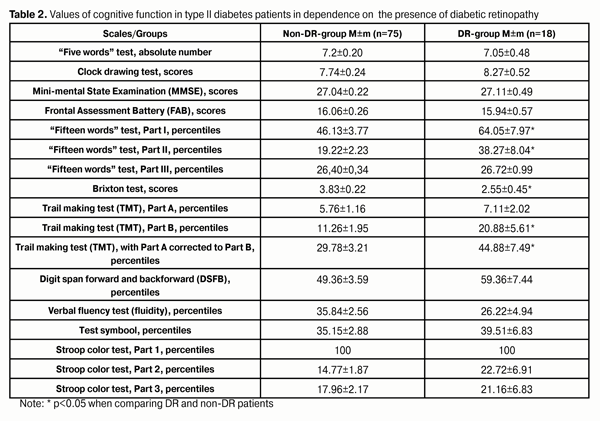
As it can be seen in Table 2, no significant difference was found in cognitive function between groups of patients according to FAB, MMSE, the clock drawing test, the “five words” test, the Verbal fluency test, DSFB, the Stroop color test, and the Тest symbооl. At the same time, when performing the “fifteen words” test, which is similar to the “five words” test, it was significantly better performed by patients in DR-group. Thus, short-term and long-term memory was in a significantly better condition in DR patients than in non-DR patients, while recognition function did not differ in the groups.
This test is very sensitive and useful for assessing the verbal learning and memory, including proactive inhibition, retroactive inhibition, retention, encoding, and subjective organization. It can be supposed that, in patients with DR, other, i.e. aural, ways for memorizing are activated due to vision impairment. On the other hand, when performing TMT, which can assess visual search speed, perception, speed of processing, working memory, and general intelligence, the better results were obtained in non-DR group of patients. Thus, TMT Part A, which can assess visual processing speed, revealed no difference between groups; however, TMT Part B showed significantly better results in non-DR-group of patients, so this group patients had better working memory and mental flexibility. TMT BA can assess visuoperceptual and working memory, providing a relatively pure indicator of executive abilities [11, 12, 13], which also were better in the non-DR-group. Poor performance of this test by DR-group of patients showed that they had more pronounced lesions in the frontal area as compared to non-DR patients. The Brixton test confirmed significant impairment in executive functions in DR-group patients in comparison with non-DR patients. Executive functions are cognitive processes which control other kinds of the brain activity and mainly activate prefrontal regions of the frontal lobes. These functions are responsible for initiative, consolidative, regulative, verbal, motional and emotional processes [14]. In turn, these processes are the basis for such functions as planning, self-feeling, problem solving, strategy selecting or sequence of behaviors for achievement of chosen goals [1, 4, 5]. This is very important since DM patients are patients with a chronic disease and have to make every-day decisions about self-control and antihyperglycemic therapy which is crucial for DM compensation and disability relief. Conclusions 1. Relationship between the presence of DR and impairment of cognitive functions in type 2 diabetes patients was revealed. 2. The patients with DR had worse rates of working memory and memory flexibility as well of executive functioning according to the TMT and the Brixton test. 3. Poor performance of the TMT and the Brixton test by the DR patients indicated the lesions in frontal and perifrontal areas of the cortex. 4. The Brixton test is recommended to perform in order to screen cognitive impairments in type 2 diabetes patients with DR since this test seems to be more sensitive and easy to perform. It can be used in patients who have problems with counting and reading.
References 1. Rury R Holman, Sanjoy K Paul, M Angelyn Bethel, David R Matthews and H. Andrew W Neil. 10-Year Follow-up of Intensive Glucose Control in Type 2 Diabetes. Engl J Med 2008; 359:1577-89 2. Cukierman-Yaffe T, Gerstein HC, Williamson JD, Lazar RM, Lovato L, Miller ME, Coker LH, Murray A, Sullivan MD, Marcovina SM, Launer L J. Relationship between baseline glycemic control and cognitive function in individuals with type 2 diabetes and other cardiovascular risk factors: the action to control cardiovascular risk indiabetes-memory in diabetes (ACCORD-MIND) trial. Diabetes Care. 2009;Feb32(2):221-6. 3. Ryan CM, Geckle MO, Orchard TJ. Cognitive efficiency declines over time in adults with type 1 diabetes: effects of micro- and macrovascular complications. Diabetologia 2003;46:940–8 4. Crosby-Nwaobi RR, Sivaprasad S, Amiel S. The relationship between diabetic retinopathy and cognitive impairment. Diabetes Care. 2013;36:3177–3186 5. Nguyen TT, Wang JJ, Sharrett AR et al. Relationship of retinal vascular caliber with diabetes and retinopathy: the MultiEthnic Study of Atherosclerosis (MESA). Diabetes Care. 2008;31:544–9. 6. Roberts RO, Geda YE, Knopman DS et al. Association of duration and severity of diabetes mellitus with mild cognitive impairment. Arch Neurol. 2008;65:1066– 73. 7. Ding J, Patton N, Deary IJ et al. Retinal microvascular abnormalities and cognitive dysfunction: a systematic review. Br J Ophthalmol. 2008;92:1017–25. 8. Crosby-Nwaobi R, Sivaprasad S, Forbes A. A systematic review of the association of diabetic retinopathy and cognitive impairment in people with type 2 diabetes. Diabetes Res Clin Pract. 2012;96:101–10. 9. Jie Ding, Mark WJ Strachan, Rebecca M Reynolds, Brian M Frier et al. Diabetic Retinopathy and Cognitive Decline in Older People With Type 2 Diabete. The Edinburgh Type 2 Diabetes Study. Diabetes. 2010;Nov 59(11): 2883-9. 10. Strauss E, Sherman EM, Spreen O. A Compendium of Neuropsychological Test: Administration, Norms and Commentary. Oxford: Oxford University Press. Retrieved 14 July 2013. 1240 p. 11.Gaudino EA, Geisler MW, Squires NK. Construct validity in the Trail Making Test: What makes Part B harder? J Cli n Exp Neuropsychol.1995;17 (4):529-35. 12.Reitan RM. The relationship of the Trail Making Test to organic brain damage. Journal of Consulting Psychology.1955;19:393-4. 13.S?nchez-Cubillo, Peri??ez JA, Adrover-Roig D, Rodr?guez-S?nchez JM, R?os-Lago M, Tirapu J, Barcel? F. Construct validity of the Trail Making Test: role of task-switching, working memory, inhibition/interference control and visuo-motor abilities Journal of International Neuropsychological Society. J Int Neuropsychol Soc. 2009;May 15(3):438-50. 14.Allison AM Bielak, Laura Mansueti, Esther Strauss, Roger A. Dixon. Performance on the Hayling and Brixton tests in older adults: Norms and correlates. Archives of Clinical Neuropsychology. 2006;21:141–9.
|