Prediction of inpatient treatment duration for cataract patients according to their clinical and social status
M.I. Kovtun1, Cand. Sc. (Med.)
M.L. Kochina 2, Prof., Dr. Sc. (Med.)
1 Hirchman Kharkiv City Clinic Hospital No 14
2 Kharkiv Medical Academy of Post-graduate Education
Kharkiv, Ukraine
E-mail: kochinam@inbox.ru
The purpose of the paper was to ground and to develop a model for predicting the duration of inpatient treatment of a cataract patient. We surveyed 60 cataract patients applied for surgical treatment in Hirchman Kharkiv City Clinic Hospital No 14. A questionnaire consisted of several question pools answering which made it possible to assess a social state of patients, somatic and ophthalmic status, features of main disease as well as the duration of inpatient stay after surgery. If the duration of stay in hospital was 0-1 day, it was considered that one day surgery was performed.
Fuzzy logic was used to design a model for prediction of inpatient treatment duration on the ground of findings of the questionnaire survey. A method of mountain clustering was used to obtain fuzzy rules.
The most informative parameters for predicting the patient’s in-hospital stay duration after cataract surgery are age, finances, the number of concomitant somatic and eye diseases. To solve the tasks of clustering, optimizing and fuzzy inference, Scilab software package with sciFLT extension package can be used.
Key words: cataract, outpatient treatment, prediction, fuzzy logic
Present-day trends in organizing eye care for cataract patients are the crossover to out-patient treatment and one day surgery [1, 8, 9]. To-date, such an approach is a standard in the organization of treatment for cataract patients [1]. The crossover to outpatient cataract treatment decreases the necessity in bed capacity, leads to energy and material resource savings, and significantly decreases emotional, physical, and financial expenditure of a patient. Otherwise, considering local contexts in Ukraine, equipment and material procurement of medical institutions and medical and social characteristics of cataract patients (elderly age, the presence of concomitant pathology, finances, place of living) make outpatient treatment not always acceptable. Patients with age-related cataract can refuse outpatient treatment motivating that they are afraid of surgery, have transport and mobility difficulties, and remoteness of the place of living from hospital. The patients’ psychological state of mind, their awareness of disease’s features and possible complications play an important role when choosing inpatient or outpatient treatment. In this regard, crucial is the role of policlinic’s specialists who should have the patients been aware of their condition and possible variants of cataract treatment [5].
In private health care facilities, cataract treatment is commonly outpatient and a patient is made for home in a few hours after surgery. It is not always convenient due to the reasons listed above. Some clinics have accommodation and meal services or hotels where the patients and attendants can stay overnight. However, this service is available far from everywhere.
There are a great number of reasons according to which inpatient cataract treatment is preferable. Among them are elderly age of patients, difficulties in their mobility, their living far from hospital (for instance, in a region or in other town), their living separately from relatives, the absence of physical assistance, reduced circumstances, and the presence of concomitant somatic pathology that can lead to postoperative complication development [2-4,6]. Moreover, an essential role in choosing a treatment type plays an ophthalmic status of the patient, the presence of concomitant eye diseases that add to the risk of postoperative complications requiring long hospital stay [2, 4, 6, 12].
Thus, a problem of choice between inpatient and outpatient treatment of cataract is conditioned by a variety of medical and social causes which must be considered in optimization of functional and organizational system of eye care to cataract patients in the context of reforming the health care system in Ukraine.
The purpose of the present paper was to ground and to develop a model for predicting the duration of inpatient treatment of a cataract patient.
Object and methods
To develop a model for prediction of the impatient treatment duration, we surveyed 60 cataract patients applied for surgical treatment in Hirchman Kharkiv City Clinic Hospital No 14.
We designed a questionnaire with several question pools answering which made it possible to assess a social state of patients, somatic and ophthalmic status, features of main disease as well as the duration of inpatient stay after surgery. If the duration of stay in hospital was 0-1 day, it was considered that one day surgery was performed.
We received answers to 39 questions while processing the questionnaires, which made it possible to take the history, to assess the somatic and ophthalmic status, social and financial situation, the place of living and its farness from hospital, to reveal the presence of chronic diseases in patients (ischemic heart disease, hypertension, diabetes mellitus, arthropathy, respiratory diseases, thyroid disorders, gastrointestinal diseases, kidney diseases and other conditions). Besides, there were questions regarding systematic alcohol consumption and smoking.
Also, the questionnaire included questions about the living place of the patients and the possibility for their outpatient treatment. These questions were very important since the main part of the patients surveyed were people of elderly and old age who had a good few of concomitant pathology and who, in some cases, required physical assistance for a hospital visit. After outpatient surgery, the patients are required to attend a medical institution for a few days to control the condition and to correct the treatment.
A group of the patients surveyed consisted of 19 men, aged 26 to 82 (mean age (63.7±16.7)), and 41 women, aged 32 to 85 (mean age (67.6±10.2)). Of the patients surveyed, 48 (80%) were persons over 60 y/o; of the latter, 24 (50 %) were over 70 y/o.
Fuzzy logic was used to design a model for prediction of inpatient treatment duration on the ground of findings of the questionnaire survey [7, 10]. In the modern practice of intellectual data analysis, fuzzy inference systems can successfully meet the challenges of modeling complex systems, designing classifications and predicting models. Any fuzzy inference system is based on a complex of fuzzy rules of knowledge base and membership function. Fuzzy rules can be obtained by an expert-analyst according to his personal knowledge or in a result of experimental data processing. Fuzzy rules, for instance, can be obtained using cluster analysis. All existing models of clustering, i.e. models for grouping a set of objects according to certain properties, can be divided into two categories: hard and soft clustering [7]. Hard clustering (non-fuzzy clustering) enables to group a set of objects into some non-crossing groups (clusters) in such a way, that each object belongs to exactly one cluster. Soft clustering (fuzzy clustering) is a form of clustering in which an object can belong to more than one cluster to a certain degree. Clustering algorithms can require presetting a number of expectable clusters or their number is defined during the course of performance on the basis of input data distribution.
The mountain clustering method presented by Yager R. and Filev D. was used to design a predicting model for the learning fuzzy rules. This method does not require the preset of the expected number of clusters. Firstly, points that can be the centers of the clusters are detected to which the cataract patients are related. Secondly, a potential value is calculated for each point, which shows the possibility of cluster formation in the area of the point. The denser the distribution of the objects (data of the patients) in the area of the potential cluster centre the more is its potential value. Afterwards, iteratively, the cluster centers are selected among the points with the maximal potential [14].
Before performing the fuzzy clustering of characteristics of cataract patients, corresponding indices had been calculated to consider their physical and ophthalmic status. Somatic condition index (SCI) was calculated as a total of scores assigned for the presence of each concomitant condition. The higher is the value of SCI the worse is the physical condition of the patient. Likewise, ophthalmic index (OI) is a total of scores for each concomitant eye disease of the patient.
Preliminary processing of data obtained from the questionnaires and patient histories showed that the most informative for the prediction of inpatient stay after cataract surgery are characteristics as follow: age, finances, SCI, OI. Therefore, a text learning sample was formed in a rectangular matrix, in which each raw corresponds to a set from one patient data; and each column contains the information about the patients as follows: age, finances (three grades: good (one score), satisfying (two scores), unsatisfying (three scores), OS and SCI values, a number of inpatient stay days.
Scilab software package [13] with sciFLT extension package [11] was used for tasks of clustering, optimization and fuzzy logic inference. The system has been developed by specialists of French Institute for Research in Computer Science and Automation (INRIA) and is distributed under CeCILL free license. Scilab system is made, first of all, for numerical computations and matrix work; it includes programming tools and has the syntax of the embedded language similar to MATLAB. Complex computation procedures such as clustering, fuzzy logic inference were supported using extension software packages through ATOMS Extension Package Manager.
Results and discussion
Analysis of the questionnaires offered to cataract patients showed that 51 ((85±4.6)%) were urban and only 9 ((15±4.6)%) were rural people. Such a distribution on the living place is conditioned by the fact that the survey was performed in a municipal, not regional, hospital. 33 ((55±6.4)%) and 27 ((45±6.4)%) of respondents lived, respectively, far from and near to hospital. Outpatient treatment was pointed as possible by 50 ((83±4.8)%) respondents and impossible by 10 ((17±4.8)%) respondents. All the patients were able to move independently.
Financial situation was marked as good only by 2 ((3.3±2.2)%), as satisfying and unsatisfying by (42 (70±5.9)%) and 16 (26.7±5.7)% respondents, respectively. Financial situation determines in many respects the possibility of the patient to visit hospital after outpatient surgery for follow-up examinations or to continue the treatment if necessary. Commonly, the patients in bad circumstances prefer to stay in hospital where they can get 24-hour qualified medical care, meal, and nursing.
Ophthalmic status was assessed through analysis of the questionnaires and patient histories. The presence of high myopia, glaucoma, retinal and optic nerve diseases were revealed in patients. Besides, a type of cataract (age-related, traumatic, complicated, radiation, toxic, systemic disease-related, congenital) and a degree of cataract maturity were taken into account. Of the respondents, there were 13 ((21±5.2)%) patients with high myopia, 11((18±4.9)%) with glaucoma, 9 ((15±3.5)%) with retinal diseases, and 4 ((7±3.3)%) patients with optic nerve disease. 31 ((51±6.4)%) patients had no eye disease apart from cataract; 23 ((38±6.2)%), 4 ((7±3.3)%)), and 2 ((4±2.5)%) patients had one, two, and three concomitant diseases respectively. Analysis of cataract concomitant eye diseases showed that the most common diseases were myopia and glaucoma, ((39±6.2)%) of respondents.
Distribution of the patients according to the type of cataract is as follows: age-related, 50(82±4.9)%; traumatic, 1(2±1.7)%; complicated, 3 (5±2.8)%; radiant,1 (2±1.7)%; toxic, 0; related to other diseases, 2 (4±2.5)%; congenital (5±2.8)%. So, most of respondents had age-related cataract (82%).
According to cataract maturity degree, the patients were distributed as follows: early, intumescent, and mature cataract was noted in 8 (13±4.3)%, 37 (60±7.8)%, and 16 (27±5.7)% patients, respectively.
The structure of concomitant conditions in patients surveyed was assessed and the most common diseases revealed were ischemic heart disease and hypertensive disease, in 35(57±6.4)% and 38(62±6.3)% of respondents, respectively. Moreover, 28 (46±6.4)% and 7 (11±4.0)% patients had arthropathy and diabetes mellitus, respectively. There were also respiratory diseases noted in 14 (23±5.4)% patients, thyroid disorders in 8 (13±4.3)%, gastrointestinal diseases in 15 (25± 5.6)%, and kidney diseases in 10 (16±4.7)% patients. In most parameters, our data on concomitant diseases coincide to those that we have obtained previously [4,6]. Assessment of somatic diseases is of a special importance for an issue of outpatient treatment acceptance since the presence of pathology and systemic intake of various medications can lead to postoperative complications to occur. When computing SCI we determined that 9 (16%) patients had no concomitant disease, i.e. SCI=0. One concomitant disease was in 8 (13%) patients; two, three, four, and five concomitant diseases were in 11(18%), 14 (23%), 9 (16%), and 5 (8%) patients, respectively; six and seven concomitant diseases were noted in 2 (3%) patients each. Thus, two and more conditions were concomitant to cataract in 71% of respondents, which points to high risk for postoperative complication occurrence and to the need for inpatient treatment.
After a learning test sampling was created in a form of a matrix, we performed a procedure of synthesis of a predictive model with initial parameters of mountain clustering algorithm as: radii = 0.5; accept ratio = 0.5; reject ratio = 0.15. To reduce the number of rules in knowledge database (this can be achieved by reducing the number of clusters), we set a reject ratio parameter of the algorithm. In this regard, a value of the reject ratio parameter was cyclically increased from 0.15 to 0.49 with a step of 0.01 and the procedure of predictive model synthesis repeated. Setting was terminated when the quality of prediction was deteriorated to a level of mean error ? > 0.5 or a minimal value for number of rules was achieved.
A block-scheme for the procedure of synthesizing an inpatient treatment duration model on the basis of Sugeno fuzzy inference is given in Figure 1.
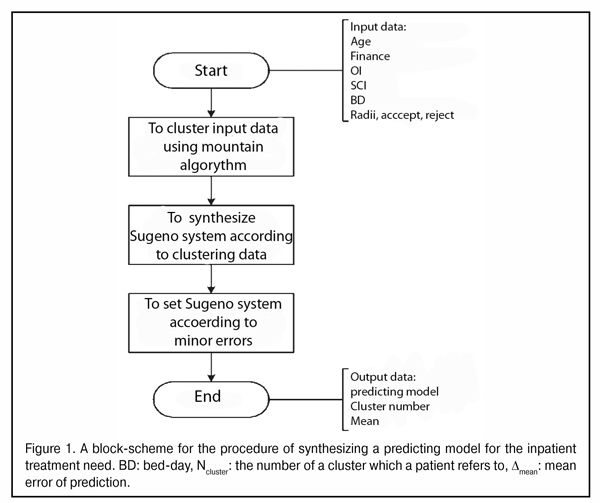
The procedure performed resulted in having a predicting model for the inpatient stay duration, a number of clusters and a value of mean error of the prediction ?mean. Parameters of the mountain clustering algorithm were as follows: a parameter determining the cluster size, radii = 0.5; suppression ratio = 1.25; accept ratio = 0.5; reject ratio =0.4.
To synthesize fuzzy rules on the basis of clustering, each cluster is assigned one fuzzy rule in the form “IF х = х’, THEN y = y’” where х is an input value of the parameter, y is an output value of the parameter, х’, y’ – fuzzy terms «ABOUT х», «ABOUT y». Coordinates of membership function maximums are accepted equal to cluster centers obtained. Membership functions of these fuzzy terms are defined by the two-tailed Gaussian function. Afterwards, a search for optimal parameters of squash-stretch of the membership functions and coefficients of fuzzy knowledge base rule conclusion is performed.
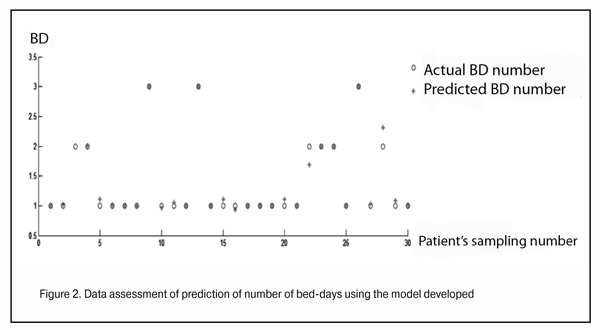
To assess the adequacy of the predictive model developed we used an approach as follows: a raw corresponding to a dataset of the one patient was extracted from the learning sample and the model was resynthesized; predicting impatient treatment duration was computed for each set of parameters (data of one patient) in the sampling. Such validity showed that the number of days of patient’s actual staying in hospital and those obtained using the predicting model agreed significantly (Figure 2).
To use the fuzzy model for predicting the inpatient treatment duration for cataract patients in the practice, it is necessary to set up Scilab system with sciFLT package extension on the personal computer and save on the hard disc as «prediction_model.fls». Thus, to obtain the prediction, it is necessary to use only two commands that are entered in the Scilab command box (Figure 3).
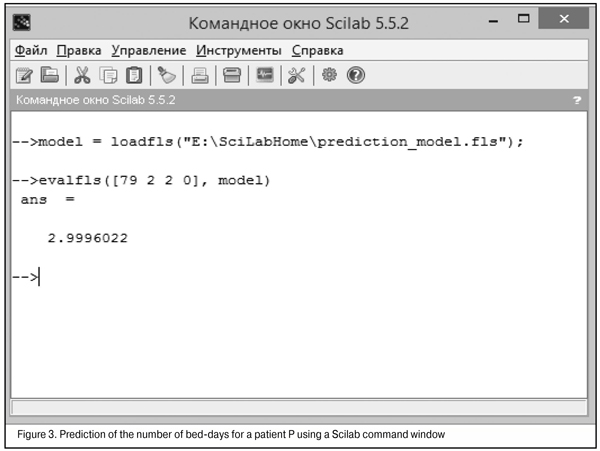
A command «model = loadfls("E:\SciLabHome\prediction_model.fls");» download the fuzzy prediction model (saved on the hard disc as a file«prediction_model.fls») into Scilab internal storage and save in a variable «model». The following command « evalfls([хххх], model) » performs a computation of the number of inpatient stay days.
Figure 3 demonstrates the use of the model developed to predict the number of bed-days for a patient P. A patient aged 79 y/o with satisfying finances (2 scores) had two concomitant eye diseases (OI=2) and no concomitant somatic pathology (SCI=0). In the figure, patient’s data are shown with a note « evalfls([79 2 2 0], model) ». The patient stayed in hospital for three days. Predicted number of bed-days was 2.9996022 days, which corresponds the actual duration of inpatient treatment.
Thus, the inpatient treatment duration prediction model developed can be used to assist in physician’s decision making in regard to cataract treatment tactic. When prediction bed-day values exceed 1, a patient should be proposed inpatient treatment; otherwise, a possible risk of postoperative complication occurrence, which can be burdened by ophthalmic and somatic status of the patient, should be considered in outpatient treatment.
Conclusions
1. The crossover to outpatient treatment of cataract reduces the need in bed capacity, leads to energy and material resource savings, and significantly decreases emotional, physical, and financial expenditure of a patient. However, it has some limitations in Ukraine.
2. The limitations for outpatient cataract treatment are: old age of patients, mobility difficulties, living far from hospital, separate living, the absence of physical assistance, poor circumstances, the occurrence of concomitant somatic and eye pathology.
3. Ophthalmic status of patient, the presence of such concomitant eye conditions as high myopia, glaucoma, retinal and optic nerve diseases play a crucial part when choosing a type of treatment (in- or outpatient).
4. The most informative parameters for predicting the patient’s in-hospital stay duration after cataract surgery are age, finances, the number of concomitant somatic and eye diseases.
5. To solve the tasks of clustering, optimizing and fuzzy inference, Scilab software package can be used, which makes it possible to predict the inpatient treatment duration for cataract patients on the basis of the informative parameters.
References
1. Cataract. Unified clinical protocols on evidence-based medicine. 2015.
Crossref
2. Kovtun M. I. Gender Peculiarity Analysis of Periods of Surgical Treatment Seeking in Case of Cataract. Vestnik problem biologii i meditsiny. 2012;(2(95))(4):91-95. Russian.
3. Kovtun M.I. Sociomedical Characteristics of Cataract Patients. Vestnik problem biologii I meditsiny. 2015;(3(120))(2):135-139. Russian.
4. Kovtun M.I The peculiarities in organizing ophthalmological care for cataract patients in conditions of reforming health care system of Ukraine. Arkhiv oftalmologii Ukrainy. 2015;3(2):14-9. Russian.
5. Kovtun MI. Level of patients’ information awareness of cataract. Aktualni problem suchasnoi medytsyny: Visnyk Ukrainskoi medychnoi stomatologichnoi akademii. 2015. 15(3-2(51)):132-6. Russian.
6. Kovtun M. I. Results of Structure Assessment which Accompanying Morbidity of Cataract Patients. Vestnik problem biologii I meditsiny. 2012;(1(96))(4):120-4. Russian.
7. Leonenkov AV. Fuzzy modelling in MATLAB and fuzzyTECH. BKhV-Peterburg: SPb; 2005. 736p. Russian.
8. Rykov SO, the Editor. Organization of eye care in modern times: a reference book for physician. Edited by. Kyiv: Doctor Media; 2008. 357p. Ukrainian.
9. Unified clinical protocol of primary, secondary (specialized), tertiary (highly-specialized) medical care. Cataract. Order of Ministry of Health of Ukraine No 49 from January, 28, 2016.
Crossref
10. Shtovba S. Design of Fuzzy Systems with MATLAB. Goryachaya Liniya - Telekom: Moscow.- 2007.- 288p. Russian.
11. Fuzzy LogicToo lbox. [Internet].
Crossref
12. Kovtun M.I. Assessment result of cataract stages distribution and concomitant diseases structure. East European Scientific Journal.2016; 1(6):48-52.
13. Open source software for numerical computation. [Internet].
Crossref
14. Yager R, Filev D. Essential of Fuzzy Modeling and Control. JohnWilley&Sons, 1994. 388 p