J.ophthalmol.(Ukraine).2016;6:43-58.
|
https://doi.org/10.31288/oftalmolzh201664357 Adaptive myopia. Part 1. Actuating mechanisms of optic axis growth in the incremental retinal defocus theory 1Petercom-Networks / Management Systems Consulting Group Cl. corp., St. Petersburg, Russia; The modern theory of acquired myopia (the theory of retinal defocus) is being considered against the backdrop of the global pandemic forecast: about 5 billion by 2050 year. The inconsistency of tincremental retinal defocus theory in part of the proposed executive mechanisms has been revealed. Until the regulations for visual work are absent, the issues of video ecology and total prevention of acquired myopia should take the first place in the fight against the myopia pandemic. Key words: adaptation, acquired myopia, defocus theory, video ecology, visual performance, control mechanisms of accommodation and axial length Introduction According to reliable prediction (2016), prevalence of acquired myopia (AM) would reach 5 billion people by 2050 that would make up 50% of global population [87]. Actually, we expect the most mass epidemic in the history of mankind, myopia pandemic. The first cause of this unfavorable prediction is likely the fact that the mankind has never had a single efficient theory enabling to prevent from AM development [29,33-45,53,59-66]. The second cause which is more global is the absence of visual work regulations for video safety of modern video media, which mean statutorily prescribed requirements to electronic data storage devices with different sized displays and different physical illumination as well as requirements to brand new energy-saving light sources, virtual individual video-glasses and video-helmets, 3D cinemas etc. in regards of visual work comfortability [22,25,30,38-44,70,77]. Actually, the mankind has become a hostage to manufacturers of video equipment and modern artificial light sources since there are no significant ophthalmologically and psychophysiologically developed arguments against their effect on the visual organ. The participation of world manufacturing companies in compulsory financing to provide their products with video-safety is, as expected, insignificant. This can be broken only at the lawmaking level upon understanding and a good will of lawmakers in every certain country. Since the pandemic of myopia is of a global character, this is an objective worth pursuing not only for World Health Organization (WHO) but also for United Nations without mentioning multinational programs. However, this path is difficult and can be completed only if a society changes its attitude to the necessity to assess the danger of modern visual media. The mankind has already experienced such co-decision: as an example, a scientific WHO committee upon Electromagnetic Field and Human Health program has been created. There are also safety recommendations on Electromagnetic Exposure accepted by the Parliamentary Assembly of the Council of Europe in May, 2011 [91]. For example, WHO has announced a precautionary principle in assuring human safety under electromagnetic pollution conditions as a priority principle in providing safety to cell phone users, which has been actively supported by governments of some states and by European Union (EU) [91]. EU scientists have determined that the specific absorption power rated 0.3 to 2.0 W/kg affects DNA. A similar way is to go when developing video ecology standards as part myopia control. Ophthalmologists and optometrists should raise public awareness of prevention from acquired myopia developing. The fight for video-safety promises to be anything but simple, and it is unclear if the ophthalmic society will wish to be involved in it. But we all should understand clearly that it is impossible to push things along without developing precisely ophthalmic requirements to video-safety of visual activity. Video-ecology is that we all should hard work on including dissertation studies; even despite the fact that not all ophthalmologists are aware of laws of light perception, organization of visual media and psychophysiologically grounded application of hardware for public delivery of information. Let us remember, for examples, texts of presentations which sometimes are difficult to read for they are of a small Times New Roman font and of a white or yellow color on a dark-blue or blue background. This is, indeed, one of the most difficult colour combinations for vision. To ease reading, such text should be printed with a visually comfortable 12 sized Calibri font rather than Times New Roman which is the most difficult to read in Cyrillic characters. But we persistently perform the paperwork using this “myopizing” font which is similar to hard-to-scan hieroglyphic symbols of Southern and Eastern Asia. Paradoxically, but school textbooks in STEM (science, technology, engineering and mathematic) science are printed with an Arial font since human science textbooks use dangerous Times New Roman. Except that, the color of the text is black instead of visually comfortable dark-blue on the white background. One should pay attention to the way how the websites of main internet search systems are designed: they mainly use blue Arial on the white background. After all, it is so easy to set this option in our personal computers. But, as a rule, we have not even heard about it. And the reason is the absence of video-safety studies on the choice of Cyrillic fonts as well as recommendations for the choice of line spacing, the necessity of hyphenation aligning line width and word spacing, and, for example, setting safe font size and type for limiting transverse diameter of phone and e-Book displays. These studies should be carried out immediately not to wrack the vision of our children at the early stage. In fact, when the half of country’s population has myopia, it will directly influence on its safety and defense capacity. This is because of the absence of wide research in video-ecology that we have an order of Ministry of Education of Russian Federation about the compulsory implementation of e-pads and e-books at schools beginning from 2015; we also have known from mass-media of a program of large-scale implementation of video-unsafe first generation LED lamps into the lightening of pre-school and school institutions, which is being prepared by manufacturers of RF Ministry of Energy [25]. Even these two beginnings, not supported by deep interdisciplinary researches of their video-safety, enable, to our opinion, to accelerate significantly myopisation of young population of RF. We should note that we all aware of high efficacy of medical room sterilization with ultraviolet emission. And when the room is lit with first generation LED lamps, there is a significant excessive dose of blue light which can cause relative changes in retinal light perception and errors of accommodation system. Besides, the excessive dose of blue light can speed up by 10-15 years the development of age-related macular degeneration (AMD), induce general somatic and physiological problems [12,25,94]. It should be added that, in 20016, American Medical Association (AMA) has prepared the report on LED-based lighting, warning the publicity of the danger of In-Ga-N-based first generation LEDs which are widely used for illuminations in towns [93]. In particular, light pollution of large metropolitan cities has been assessed (Fig. 1).
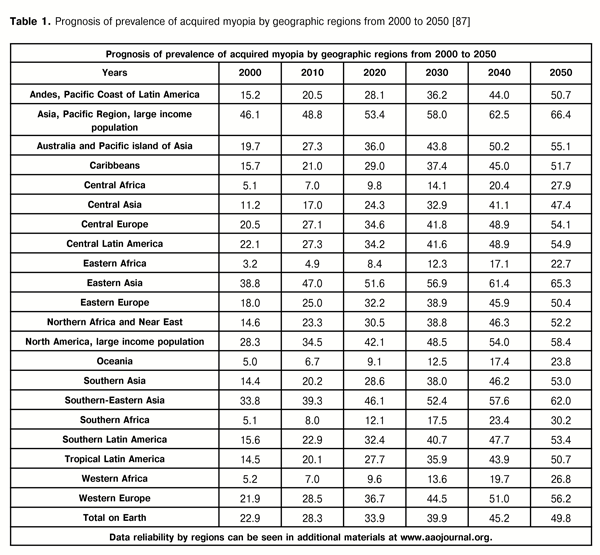
A degree of visual fatigue of an operator during the work with videoterminals cannot be assessed without considering their frequency and contrast characteristics [13, 30, 46, 52, 77, 80-85]. “Thus, for example, it has been shown that band adaptation of the visual system to line spatial frequency and to time display flicker frequency leads to operator’s fatigue. An apparent negative effect of beats between display flicker frequency and flicker frequency of luminescence lamps of general lighting has been shown. So, mass implementation of these energy-saving light sources in rooms with display equipment leads to excessive load and unavoidable loss in the main issue, the human’s state” [50]. Since the influence of LED lighting on the human health at different age are understudied and remote risks of this influence have not been assessed, an Act No115 from 29.11.2014 of Ministry of Health of Belarus says: “Application of LED light resources is not allowed for artificial lighting of educational institution rooms in which educational process is held and of functional rooms of health care organizations”. And today, a national program on research in this field is being financed in Belarus. All problems mentioned above refer to the global task, a creation of visual work regulations, without solving of which it is impossible to fight AM out since, to our opinion, AM is, first of all, an adaptive process. But, even today, ophthalmologists can do a lot in regard to prophylaxis and prevention of AM by creating an efficient theory of acquired myopia, developing criteria for safe visual work and using a rational optical correction. Let us address the prognosis of AM prevalence by 2050 for the further understanding of the paper’s ideas [87]. Table 1 demonstrates that acquired myopia would almost reach 50% of region’s population only in Central, Eastern, and Southern Africa as well as in Oceania.
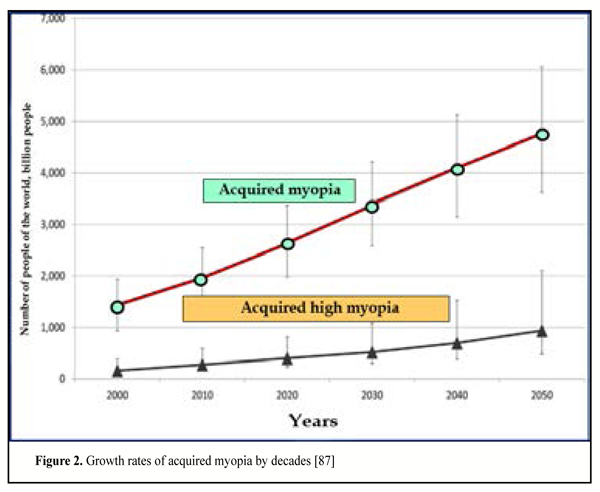
In the rest parts of the planet, more than 50% of population would have AM, with maximal rates in Pacific region, 66.4%. As for close to us Eastern Europe, AM patient rates would reach 50.4%. Figure 2 shows the prognosis for rates of AM growth by decades. These curves make it possible to conclude that 1) rates of AM spread among people of Earth would grow gradually and linearly (exponentially) and 2) among them, a relative ratio of high myopia patients would decrease.
However, bar graph analysis is uninspiring (Fig. 3). The main part of myopia patients would age 20 to 40. This means that people would not only have progression of myopia acquired at their teens but, above all, young myopes would be added by nearly the same number of mature age myopes.
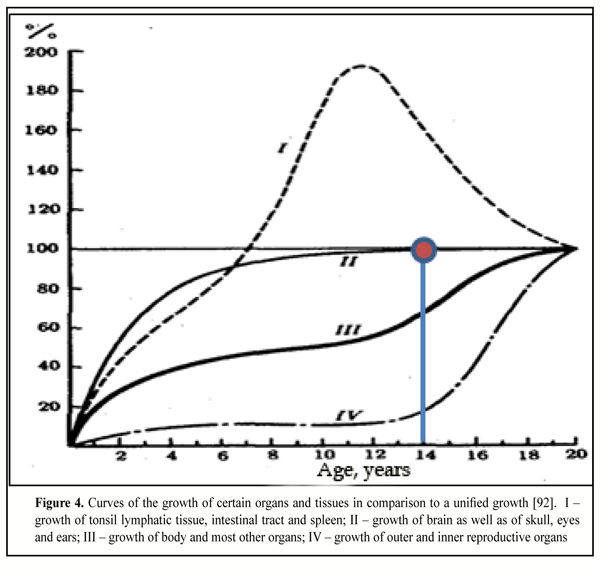
Bar graph in Figure 3 shows that, beginning from presbyopic period according to WHO classification (45-60 y/o), a number of myopia patients in a group of older age people would increase 5-10 times as compare to the year of 2000. And this is despite the multifold possibilities of surgical and optical correction. To avoid these catastrophic tendencies, it is required, first of all, to have a credible theory of AM development. Over last hundred and half years a number of AM theories have been proposed. One of them will be analyzed in our paper. I. Incremental retinal defocus theory (IRDT) Efficiency of hypothesis. A hypothesis by G.K. Hung & K.J.А. Ciuffreda (2003) [47, 88-90] on the role of retinal peripheral defocus in regulating the axial length growth is the most discussed issue in RF today [7, 47-48, 72, 75, 76, 78]. According to this theory, hyperopic peripheral defocus (over-correction) accelerates the development of myopia, while myopic peripheral defocus (under-correction), contrary, retards its development. According to IRDT hypothesis, axial length growth is supposed to be regulated to visual environment not by central nervous system (exactly, in brain) but by the retina as a self-periphery. The result depends on the size, blur and contrast of an imagined “light spot” on the retina: herewith, the size of the spot is supposed to regulate the rates of neuromodulator-release by amacrine cells which can theoretically transmit through the pigment epithelium, Bruch’s membrane and choroid to the sclera. And this is unclear so far which contrast is meant by IRTD authors: contrast of light (retinal lighting) or contrast of color (saturation of the spectrum). Physiological mechanisms. Mechanisms and processes are variable: mechanisms of feedback of the brain to ciliary muscle while eye’s focusing (by the way, which is not entirely clear to the science), mechanisms of supposedly controlling effect of light spot contrast (rather than anything else) on the efficacy of chemical processes in the retina, and, at last, mechanisms, not described by physiologists yet, of collagen formation control in the scleral structure through neurotransmitters delivered from the retina to the sclera. The eye is considered here cybernetically [4, 8, 9] as interrelated control systems for different biophysiological processes [31, 44, 63]. But here, we would like to be clear. The fact that authors have suggested out revolutionary IRDT hypothesis is worthy of deep respect. They think! And they are not afraid of laying themselves open. The good thing about hypotheses is that they can be always tested simultaneously in different clinics, which significantly advances an approximation to the truth. This is “a discordance between focus and retinal area” that IRDT advocates give the main role to in control of axial length growth considering that “image-defocus directly regulate the growth of the eye, changing the rate of release of retinal neurotransmitters which have direct effect on proteoglycan synthesis and scleral matrix biology”. Herewith, “the main role in regulation process belongs to retinoid acid; imposed defocus has reverse effect on its level in the retina and choroid (choroidal thickness is accompanied by an increase of the content of the latter); besides, retinoid acid inhibits synthesis of scleral proteoglycans” [73]. However, careful examination of IRTD hypothesis in the part of proposed regulating mechanisms of axial increment raises a lot of complicated questions. IRTD terms and notions. Any theory introducing new terms and notions must be consistent with historical experience. Peripheral vision, providing not only detection but determination of a relative movement rate of an object aside, is of a crucial importance for subject’s survival. This physiological mechanism is required since we don’t have side binocular vision enabling to estimate immediately the distance to an object moving aside as well as its relative size. However, mechanism of peripheral vision in humans can immediately assess the movement rate of the object. And we can, for example, escape a sudden blow of a tree branch from aside or even a car. And, first of all, it is possible due to sensitivity of rods of far (60-80°) rather than near (20-30°) periphery of the retina. This is periphery of the retina-receiver that provides us with effective functioning of this important mechanism. That is way a surface of the retinal dome makes up 70% of the inner surface of the eyeball. In other words, it is incomparably larger in size than the macular with its important physiological periphery in which blue cone and rod concentration is maximal. In the far peripheral retina, rod tightness is approximately 100 times less than along macular circumfery; there is an insignificant amount of codes in the far retinal periphery. Actually, we have a significant morphofunctional difference between retinal periphery and the visual centre of the retina, the macula. According to IRDT, the peripheral retina is its far and near peripheral parts, but not its inner and outer surface in the macular area. The terms of hyperopic and myopic peripheral defocus, proposed by authors, correspond to well-known overcorrection and undercorrection. That is why the catchterm of peripheral defocus should be excluded from the national ophthalmologic practice and from regulatory documents. We have already had well-turned terms of overcorrection and undercorrection which display adequately visual processes that occur [1-6, 14-16, 19-21, 23, 24, 55, 56, 67, 81-85]. So, we will use these terms. To provide successful and long-lasting living upright activities, people usually have with-the-rule astigmatism of 1.25-1.5 D [57] which is physiologically required for effective work of the most important mechanism of non lenticular astigmatism: the ability to determine quickly a vertical size of a front object when a reflex (slower) ciliary muscle (CM) is not involved yet [26, 32, 37, 63]. The vital task to detect early a vertical size of hazard can be quickly solved not only by physiological astigmatism of 1.2-1.5 D in vertical meridian but also by a comparative analysis of the optic signal from simultaneously upper and lower receptors in the peripheral retina which are located far from each other. We should note that, for example, a tortoise apart from CM has also an extra cross-striated (i.e. quick) muscle to change immediately refractive capacity of the eye in vertical meridian [79]. So, with-the-rule physiological astigmatism of 1.25-1.5 D is surely useful and full correction of essential regular with-the-rule physiological astigmatism, which is used by some optometrists, is perplexed and regrettable. Refractogenesis. This issue, regretfully, is rather complicated in modern ophthalmology. IRDT hypothesis argumentation includes some experimental data on closing plus and minus lens to chicken’s and animal’s eyes developing at early ontogenesis period, which is supposed to lead to the development of hyperoptic and myopic refraction. We will not assess the integrity of these experiments. The important thing is that, to IRDT hypothesis authors’ opinion, a controlling effect of optic action on “the genetic process of refractogenesis” is evident [47]. However, there are early and late refractogenesis. Although physiological mechanisms and differences of these stages are understudied, they are significant [57]. Early refractogenesis. The period of early refractogenesis is characterized by conformable growth of the skull, orbit and eye ball in accordance with individual genetic code. The difference in growth rates of human organs and tissues are given in Figure 4 [92]. Figure 4 demonstrates summarized age curves for: growth of tonsil lymphatic tissue, intestinal tract and spleen (I); growth of brain as well as of skull, eyes and ears (II); growth of body and most other organs (III); growth of outer and inner reproductive organs (IV) [92]. It is well seen that genetic growth of the eye in humans stops by 14 years old (red dot). However, IRDT authors suggest considering that this biological law is not observed in billions of people. The eyes (and maybe other organs) of these billion people should have the possibility of accelerated axial length at the genetic level from teens to presbyotic age. But there is no clinical evidence of such approach so far. There is only a hypothesis.
Figure 4 shows that, contrary to early childhood (2 to 5 years), the growth of the eye is genetically retarded at the age of 10-14 years so it cannot provide a quick axial length control directly without any other mechanical, rather than biochemical, operating mechanisms involved. This is because axial growth of the eye should be accelerated by times as compared to relatively slow down growth of the body and brain in early youth. And this is here when we would notice the main issue in IRTD hypothesis. “Authors suggest that there is a biochemical mechanism controlling axial length growth in the retina. This mechanism, in response to changes in retinal-image defocus, can alter natural genetically-programmed growth of the eye” [47]. IRDT hypothesis suggest that outer optic environment can control (accelerate by times) a genetic program of axial growth. This suggestion itself is in basis of the theory of incremental retinal-defocus which is supposed to influence strongly on the rate of genetic control of axial length even till the presbyopic period. It is known that a genetic program of gradual growth of the eye in all directions and according to parallel growth of the skull and orbit is put in each child. And this program will be performed even if we cut the optic nerve. And, the child’s eyes in norm will definitely reach the condition of mild hyperopia [28. 74]. This condition ends early refractogenesis in norm: eyes are grown simultaneously with the body and inner organs. In children with inherited predisposition, a genetic weakness of the process of collagen formation in the fibrous tunic of the eye can lead that hyperopic “initial stage” would be passed as early as at early refractogenesis stage; and the axe of such eyes, over early genetic refractogenesis, would be longer because of bad inheritance. Axial length of the fast-growing child’s eye will prevail in such eyes since, by then, there are no other directions for the eye to grow. Thus, beginning from the period of early refractogenesis, the child starts not with mild hyperopia but, for instance, with mild myopia. (This is, likely, inherited progressive myopia). Late refractogenesis. This period refers to the age of 14-23 y/o and is known rather poorly. There are a few clinical data on its comparison with the period of early refractogenesis; and these data confirm the possibility of far more quick growth of axial length at this period [57]. This requires additional fast control for hazard detection visual mechanism which is the same for the whole animal world. And this is a key question in “philosophy” of acquired myopia development: if the mechanism of accelerated visual “axial” genetics does not work in children, teens, and adults, so which operating mechanisms cause mass and fast AM occurrence and development in their eyes? It’s more likely that adaptive AM develops quickly with the help physiological operating mechanisms, rather than genetic, and even in early teens against the background of the normal genetic growth of the eye, though slow down by then, and even in adults [68, 80, 85]. It should be noted that some of revolutionary ideas of IRDT have been a step forward for science since increment of axial length is suggested to consider as genetically-controlled regulation process. That’s why IRTD advocates have started to search for operating mechanisms of targeted accelerated affect on the genetic code. And thus, it has been impossible to avoid involving possible biochemical mechanisms so far. However, IRDT supporters could not represent AM as an adaptive process for, in that case, AM would be considered as adaptive reaction to visual environment but not a disease. After all, adaptation or uncontrolled growth of the eye? Probably, the authors and advocates of IRDT have not taken into consideration adaptive operating mechanisms regulating axial length growth regardless to heredity. In 1965 V.N. Sorokin and E.S. Avetisov first concluded in their theory of myopia development that “myopia should be considered as a result of adaptive reaction and a case of progressive myopia as a result of over-regulating when a reasonable process turns into its contrary” [51]. Despite the depth of investigations performed to prove this bright hypothesis [1-6], E.S. Avetisov ran out of time to find an operating mechanism for controlling axial length rate according to visual load; although, to our opinion, he was about. Sorokin-Avetisov theory, which connects visual loads, accommodation insufficiency (unfortunately, the weakness of the whole accommodation system rather than tiredness of the ciliary muscle only) and genetically inherited weakness of the sclera, was just a breakthrough in the area, generalizing a wide range of national and foreign AM hypotheses. These are, first of all, hypotheses by V.I.Dobrovolskii (1868) [26], A.I. Dashevskii (1962-1983) [23, 24], V.V. Volkov et al. [14-19] suggesting the possible connection between visual accommodation loads and axial lengthening of the eye. To date, significant clinical experiments have revealed that, for instance, “a large value of relative amplitude of accommodation of myopic eyes discredits the idea that accommodation insufficiency is a cause of development and progression of acquired myopia in children” [54]. However, this is without prejudice to early ideas of E.S. Avetisov et al. on the mechanisms of AM development but only perfects its other more important features. AM can develop in adults, in particular, pilots of modern airplanes, submarine teams in long-lasting endurance cruise, sorters at diamond manufactories and watch factories, microscopists and other workers of visual stress work [2, 8, 17, 30, 77, 80, 83, 85]. S. A. Baranov has concluded that “professional adaptation of the eyes from functional stress occurs even in adults while performing precision work at manufactories of radioelectronics, precision instruments, jewellery industry and watch industries” [11]. This kind of adaptation also is true for workers in banking, economic and other fields of human activities connected with intensive visual stress [70]. Let us remember adaptive myopization of mature cats and dogs in small flats, of other animals in narrow zoo cages as well as, in instance, a family of apes, including gorillas, chimpanzees, orangutans, and rhesus macaques, which are forced to place “guard” around the monkey group due to acquired adaptive short-sightedness. But we can never meet “watchers” in a pack of wolves since their visual environment does not expect long-lasting work nearby: their eyes must proved excellent far sight. And, for example, an anteater needs myopia since it nearly always deals with small objects [95, 96]. It should be appropriate to recollect ergonomics and energy efficiency, a biological law of nature, according to which there is “an adjustment” to the size, anatomically consistent to the life environment, of every living thing. We should remind that ophthalmic ergonomics as a part of this law and being first implemented in the national practice by an outstanding ophthalmologist Professor Iu. Z. Rozenblium has not been called back. And at that, there have been revealed “not genetic” but physiological mechanisms of axial growth of the eye, which will be described further. Development and adaptive progression of initial AM appear to be connected with a common physiological mechanism, similar in humans and in animals [31, 33-35, 38-41, 63-64]. Formation of axial length, which would be adequate to visual stress, is to provide a possible low-energy level during the stressful and long-lasting near visual performance. An adaptive anatomic increment of axial length that occurs in initially hyperoptic eye under the conditions of near vision stress is likely an evidence of the law of energy efficiency in biological system development at all ages [32-33, 41, 44, 63]. If so, it should be concluded that acquired myopia is not a disease but normal adaptation to visual environment. Hence, only high myopia with complications would be considered as a disease. Thus, prevention and treatment of mild and moderate myopia degrees would be oriented to exclusion of physiological functional capacity of the human or animal eye to adaptive increment of its axial length. Thereinafter, we will explain this keynote and demonstrate that “acquired myopia is a classic case of preponderance of accommodation over outflow” [45]. However, if AM is an adaptive process, should we treat it? Indeed, today, all of mankind accommodate oneself actively to new conditions of visual environment. And over time, everyone would be a mild myope as early as in childhood and would be adopted perfectly to work with displays and gadgets. Though, they would never be able to stare splendid landscapes in distance without additional optics especially if it rains and a strong wind blows. The second part of the world would be lost in many ways for such homo myopicus. However, even in “myopic civilization”, refractive surgery would be still required without mentioning non-surgical methods. And this would not be medicine so far but a brand new service, ocular cosmetology, which would treat discomfort of vision in other non-display fields of human activity. Taking into account these circumstances, prevention of AM development is still of a great importance and it should be carried out even now. Operating mechanisms of axial length of the eye. According to IRDT hypothesis, the retina is a “brain center” of axial growth even if the optic nerve is cut. This is a strong but difficult hypothesis. So, animal’s eyes can quickly grow even if not connected to the brain, if a focus is set to the necessary direction. In other words, processes of early and late refractogenesis are one and undivided in IRDT: genetic mechanisms of development in children are just extrapolated to teen and adult periods. Hence, it is clear why, according to IRDT, accommodation regulation system must not be involved in adaptive increment of the axe of the eye. “…Corresponding changes in axial length rates occurred even in conditions when the optic nerve and nervous nuclei controlling accommodation were damaged, which excludes any influence of feedback mechanism at the central or cortical levels” [47]. IRDT authors have given an explanation of myopization process as follows: “since accommodation mechanism cannot compensate the most retinal-image defocus area induced by convex and concave lenses of significant optic power (in experiment in animals), the accommodation system in these experiments, basically, does not influence on the effect observed” [47]. And these ideas throw IRDT far back to the XIX century. This vulnerability of IRDT has already been noted by national researchers. In particular, “a model of refractogenesis developed by E.S. Avetisov (1986) and accepted in our country deserves high attention; in this model, accommodation plays a regulating role in this process… By the centre regulating eye growth, E.S. Avetisov meant “not anatomical but functional term, a system of neurohumoral effects, providing the growth of the eye and the guided formation of ocular refraction”. Thus, myopia can be considered as a result of adaptive reaction of the organism… in the guided increment of the eyeball putting through according to feedback principle” [7]. It is should be noted that the mankind have collected such a great knowledge about the presence of a relation between accommodation and axial length of the eye so it would not be possible for IRDT to survive through history under this “avalanche”. However, IRDT authors have made certain overtures to the mediated effect of accommodation on the axial length growth. To explain outcoms of various clinical trials on the effect of a correction degree on myopia progression in children, IRDT authors have appealed to a method of accommodation response enabling to assess accommodation system at different visual stimuli levels. “Non-linear dependence of accommodative response on accommodation stimulus amplitude is well-known. In case of full correction, accommodation system can compensate the changes in retinal-image defocus area so everything operates under the normal conditions. Retinal-defocus level is equal to the difference between stimulus level and accommodation response level. With under-correction, a decrease in retinal-image defocus area occurs when focusing from far-to-near and such a decrease in defocus provides myopia progression” [47]. This approach even more obscures IRDT hypothesis proposed. On the one hand, there is complete negation of the effect of accommodation on the axial length growth; on the other, “since bifocal and multifocal lenses provide accurate retinal-image focusing for both far and near objects, wearing these lenses, according to IRDT, must have a relatively small effect on the genetically-programmed growth of the eye”. In other words, “this is right because this is true” [47]. According to IRDT, “In the retina, there is a center-surround mechanism for regulating axial growth rate; the mechanism is sensitive to local image contrast, and, in turn, the retinal-image defocus. An increase in retinal defocus area (a change from a small to a large blur circle) increases surround excitation relatively to the center. This excitation causes an increase in the rate of neuromodulator-release by amacrine cells which are sensitive to contrast changes in the periphery” [47]. “Neuromodulators, such as dopamine, transmit this increase into an increase in nervous conduction and flow of chemicals through the choroid to the sclera. This, in its turn, causes an increase in proteoglycan synthesis which increases the integrity of the structure of the sclera. The increase in the integrity of the scleral structure retards the growth of axial length and, thus, retards myopia progression. A decrease in retinal defocus area, in contrast, results in a decrease in neuromodulator-release rate, decreases the rate of proteoglycan synthesis, decreases the scleral structural integrity, and, thus, an increase in the rate of axial length growth. This leads to myopia progression” [47]. Scientifically, all of the aforesaid is nonsense since, in IRDT, a description of clinical results is based on the diametrically opposed ideas in the meanwhile: in some clinical cases, accommodation plays in refractogenesis a role necessary for authors, not in others. Besides, “the authors suggest that chemicals can transmit through the choroid to get to the sclera. In the sclera, these agents, likely, can control the rate of proteoglycan synthesis, and, thereby, the rate of the sclera growth” [47]. This is, indeed, strong assumptions. Collagen-genesis in the sclera appears to be regulated directly by the retina which can push its chemical regulators via the layer of its pigment epithelium through the choroid and suprachoroisal space [49]; and these regulators control collagen formation of the sclera though it is unclear through what physiological mechanism. To IRDT authors’ opinion, the flow of “regulating signals from the retina to the sclera is connected to the fact that “amacrine and/or inner plexiform cells with their strong branches in the their outer layer have an effect, depending on the information level transmitted, on the other retinal layers, and in turn on other parts of the eye such as the choroid and sclera”. Brilliant! Even without the brain involved, the retina appears to be able to process and assess the level of transmitted visual information and to produce the corresponding amount of chemicals which somehow will act upon the receptors in the sclera responsible for collagen formation in the fibrous tunic of the eye. But, to our best knowledge, such kinds of physiological mechanisms have not even been discovered. And the main thing is that all this must occur without brain involved with the help of independent center of the eye growth which is in the retina. That is why IRDT hypothesis on the fact that neuromediators produced in the retina can be transmitted to the sclera via retinal pigment epithelium and regulate collagen formation rates should be confirmed clinically. Unfortunately, we have poor knowledge of trophic mechanisms in the retinal structures. It is supposed that there are two sources for retinal trophism: 1) the central retinal artery for six inner layers and 2) choriocapillary layer of the choroid itself for four outer layers of the retina. M. M. Boyer, G. L. Poulsen, T. M. Nork (2000) [86] have investigated that the pigment epithelium of the retina is a layer of epithelial cells and provides photoreceptors with nutrients. However, pathways and mechanisms of nutrients delivery from the aqueous humor in suprachoroidal space to the retina are undefined. As well as undefined are all the metabolic elimination pathways from the vitreous and retina. But what is well-known so far is a close relationship of AM degree with a site of dystrophic changes in the retina and with the possibility to retard these dystrophic changes if optical correction is chosen properly [22,45]. Conclusion “To IRDT authors’ opinion, their theory gives a simple and physiologically real mechanism which explains how high plus lenses, full correction, or under-correction in myopia progression can facilitate the changes in axial length by hyperopic, emmetropic, and myopic types, respectively” [47]. Actually, this is a hypothesis so far since there is no clinical confirmation for operating mechanisms proposed and the keynote approaches are diametrically opposed. However, we’ll try to have an open mind. 1. IRDT pros: 1.1. The obvious positive point is that the IRDT authors have appeared the understanding of a direct relation between axial lengthening and a possible failure of collagen formation in the scleral structures, which have been revealed previously by Russian scientists [1,10,33-35,37-40,51]. “Authors suppose that chemicals flow (from the retina-producer, insertion is ours) can be transmitted through the choroid to get to the sclera. In the sclera, these chemicals are supposed to be able to control the rate of proteoglycan synthesis and, thus, the rate of the sclera growth". This is another historical attempt to explain the refractogenesis of AM with the help of mismatch in the work of collagen formation mechanisms in the sclera. Though, it was reflected in 1974 in a classical dissertation by T.E. Nikolaieva [51]. And it is in 1997 when we noticed the direct relation between accommodation and outflow [18]. 1.2. The attempt of G. K. Hung and K. J. А. Ciuffreda to explain the mechanism of “eye’s focusing” through neuromodulators sensitivity to retinal-image contrast changes should be embraced by all means. This is a prospective idea though it is not the first but very important effort. In fact, we have not understood completely until quite recently how a brain/ciliary muscle feedback mechanism which changes the tension of the ciliary muscle and provides focusing is organized. We and other researchers [27] have understood that that is not “image blur” but something else which is connected with a relative sensitivity of excitation areas in the retina. And the contrast of incoming optic signal, apparently, can be one of additional factors providing a better operating effect of such mechanism. 1.3. The attempt of G. K. Hung and K. J. А. Ciuffreda to find direct operating mechanisms of the visual stress effect on collagen formation in the posterior part of the sclera is worthy of respect. Though this attempt has obviously failed, the huge meaning of it is that it creates public opinion in professional ophthalmic society and other researchers of the eye. It looks like a lot of other up-to-date parallel investigations in this scientific direction will be performed in different clinics, which will advance the understanding the nature of acquired myopia. 2. IRDT cons: 2.1. The idea of the brain not involved in the late refractogenesis goes against a great number of clinical evidence and, in prospect, would do more harm than good since a significant part of researchers would get distracted to check this physiologically incorrect hypothesis. 2.2. The hypothesis that the retina is an axial length growth center which is separated from the brain in the most incorrect. Here, we are fallen into the area of mythology staying in two-dimensional (the retina) rather than three- dimensional world of a higher control system which is called the brain with its periphery in the form of the retina-receiver. In fact, in ophthalmology, no efficient physiological hypotheses clearing the physiological principles of the control system and operating mechanisms of accommodation have been given over centuries. I. N. Koshits and O.V. Svetlova have been coming up to the formation of efficient hypotheses in this area and, perhaps, have succeeded, in some ways. This will be mentioned a bit later. 2.3. The idea itself that the retina produces and, afterwards, delivers via its own pathways chemicals providing the regulation of refractogenesis rates at genetic level have been taken, likely, from science fiction. Indeed, to date, biochemical processes in the retina have been described in reasonable detail though not in full. But we can never find the information that the retina is a biological “machine” directly controlling the growth of the sclera. Once again, let us not accuse the authors since they may, like many other ophthalmologists, be still in thrall to myths about second-ratedness of aqueous humor outflow uveascleral pathway which is the only in the eye in lots of animal species; and they do not suppose that the sclera is the main filter for waste aqueous humor elimination out of the eye. For this, in the sclera, there are prostaglandin receptors regulating its permeability and mechanoreceptors regulating the size of the eye. They are also not aware of the fact that it is the aqueous humor that is the main transmitter of metabolites which are necessary to maintain normal collagen formation in the sclera as well as normal metabolism in the retinal structures [22,31,35,44, 59,62,63]. And changes in the architectonics of the anterior segment of the sclera have not been found morphologically [10, 51]. To turn this dream into reality, IRDT authors should not only find in the retina a rather strong “mechanisms of production” of specific inhibitors and catalyzers for the sclera growth but, crucially, find out the pathways of their delivery to the sclera trough the retinal pigment epithelium. 2.4. A serious downside of IRDT is a low response rate to changes in visual environment (years) as well as the absence of easily defined ideas of the functioning of one of the reputed parts of eye growth general mechanisms mainly along its optical axe. And this is without mentioning the absence of any regard to the law of energy efficiency and ergonomics in the development of biological systems. 2.5. Understanding the courage of IRDT hypnoses proposed, in general, their obvious one-sidedness and limitation should be noted. Other possible operating physiological mechanisms of the adaptive acquired myopia development and clinical outcomes on its retardation on the basis of a metabolic myopia theory will be discussed in the following article. References
|