J.ophthalmol.(Ukraine).2016;2:9-12.
|
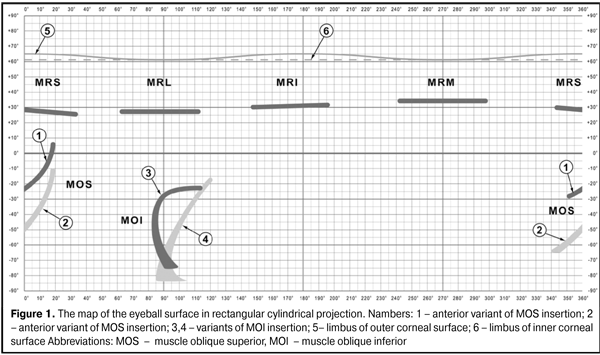
https://doi.org/10.31288/oftalmolzh20162912 Topography of superior oblique muscle’s insertion to the sclera V.I. Yemchenko, Cand. of Sc. (Med) Kremenchuk City Children Hospital Kremenchuk (Ukraine) E-mail: glmg19@yandex.ua Background. Object’s localization on the surface of the eyeball is traditionally performed by measuring the distance to other objects. These measurements are made in linear values either straight on the eyeball surface. However, the size of the eyeball in every individual is different depending on the age and refraction. When using only linear measurements, it is impossible to localize correctly any given object on the eyeball surface without regard to the eye’s size. As a rule, all distances are given for an average size eye of an adult, 12 mm in radius. Since the sizes of eyeballs of patients, especially of children, are varied depending on the age and refraction, corresponding tables of distances should be done for different eyeball sizes when localizing the zones of insertion of extraocular muscles. The purpose of the present paper was to specify the localization of superior oblique muscle’s insertion to the sclera using spherical coordinate system. Materials and Methods. 24 eyes of 19 patients were examined. Radius of the eyeballs ranged from 9.5 to 12.5 mm. The examinations were performed during strabismus surgeries. To transform the linear values into spherical coordinates, “Computed software for calculating the coordinates of objects on the surface of the eyeball model" was used. To map out anatomical formations on the eyeball surface, we created a map of the eyeball surface in rectangular cylindrical projection of ophthalmographical spherical coordinate system (OSCC). Results. Superior oblique muscles insertion sites are localized between 340° and 30° longitude and between 25° and -65° latitude. However, the major area of superior muscle insertion is between 350° and 25° longitude and between 10° and -50° latitude. Herewith, the anterior border of insertion area is mainly located within the range between 10° and 25° longitude and posterior border are scattered from 350° and 15° longitude. As for latitude, it is even more variable: there are both extremely anterior and extremely posterior variants of insertion. The relative longitude of the insertion site is also widely ranged. Conclusions. The use of ophthalmographic spherical coordinate system enables to standardize the localization of superior oblique muscle insertion sites without regard to the size of the eyeball. The possible localization of the superior oblique muscle insertion to the sclera was admeasured within the range mainly between 340° and 30° longitude and 25° and -65° latitude. Key words: superior oblique muscles, insertion, Spherical coordinate system, mapping of the eyeball surface Background Object’s localization on the surface of the eyeball is traditionally performed by measuring the distance to other objects [3, 5, 8, 9, 10, 11]. These measurements are made in linear values either with dividers straight on the eyeball surface or during ultrasound (US) and computed tomography (CT) investigations. However, the size of the eyeball in every individual is different depending on the age and refraction [1]. Thus, when using only linear measurements, it is impossible to localize correctly any given object on the eyeball surface without regard to the eye’s size. As a rule, all distances are given for an average size eye of an adult, 12 mm in radius [8, 10]. This is rather inconvenient for strabismus specialists since they deal with patients whose eyeball sizes are quite different from the “standard”. So, for example, the diameter of the eyeball in a newborn, 1-year-old, 3-year-old, 7-year-old, and 11-year-old child is 16 mm, 19 mm, 20.5 mm and 22 mm, respectively, and it can be 30 mm and more in myopia patients [1]. When localizing the zones of insertion of extraocular muscles, corresponding tables of distances should be done for different eyeball sizes [2]. The use of spherical coordinate system (SCS) to localize objects on the eyeball surface makes it possible to avoid inconveniences pointed [7]. Coordinates in SCS are specified by longitude (?°) and latitude (?°) and they do not depend on the eyeball size [7]. Thus, the corresponding tables of distances for different eyeball sizes become unnecessary. In view of the foregoing, it should be useful to specify the localization of a number of objects on the eyeball surface. A site of superior oblique muscle’s insertion to the sclera is to start with. The purpose of the present paper was to specify the localization of superior oblique muscle’s insertion to the sclera using spherical coordinate system. There were two tasks as follows: 1.To standardize the localization of superior oblique muscle’s insertion to the sclera using spherical coordinate system. 2.To admeasure the possible localization for the site of superior oblique muscle’s insertion to the sclera. Methods The investigation was carried out during strabismus surgeries. The localization of the anterior and posterior borders as well as the midpoint of the insertion site of the superior oblique muscle was determined. Dividers were used for measurements. Linear distance was measured from the limbus and from medial and lateral limbi of superior rectus muscle's insertion. A computer programme for calculation of object coordinates on the surface of the human eyeball was used to transform the linear values into spherical coordinates, [4, 6]. Preoperatively, radius of the eyeball was determined acording the data of US and CT (CT was performed in two patients). Radius was thought of as a half of equatorial diameter of the eyeball with accuracy of 0.5 mm. To map out anatomical objects on the eyeball surface, we created a map of the eyeball surface in rectangular cylindrical projection of ophthalmographic spherical coordinate system (OSCC) [7]. In this projection, parallels are figured with parallel lines and meridians are figured with equally-spaced lines perpendicular to parallels. Map scale depends only on latitude here. Lines of equal distortion coincide with parallels.
Material Nineteen patients underwent ocular examinations. All patients had different forms of strabismus accompanied by dysfunctions (hyper or hypo-functions) of the superior oblique muscles. There were 8 boys and 11 girls. Among them, there were two 2-3-year-old, ten 4-6-year-old and seven 7-14-year-old children. In primary position (PP), esotropia, exotropia and orthotropia were noted in 10, 8, and 1 children, respectively. A vertical deviation in PP was noted in 4 patients. Excyclodeviation and incyclodeviation in PP were noted in 6 and 4 children, respectively. A-pattern was revealed in 11 children; 7 children had V-pattern; 1 child had no A-V-X pattern. Total of 24 eyes (11 right and 13 left eyes) were examined. Both eyes were examined in 5 children; one eye was examined in 14 children. There were 7 eyes with low emmetropy and hypermetropy, 10 eyes with medium and high hypermetropy, 3 myopia and 4 astigmatism eyes. Radius of the eyeballs ranged from 9.5 to 12.5 mm. Results Figure 2 demonstrates the fragment of the map of the eyeball surface in rectangular cylindrical projection of ophthalmographical spherical coordinate system (OSCC) [7], which embraces the area of the eyeball between 330° and 40° longitude and between 35° and -70 ° latitude. As it can be seen on the map, the insertion site of the superior rectus muscle (black paint) is located within 25-30° latitude. Topography of superior rectus muscle insertion, like of other rectus muscles, is largely the same in different literature [3, 5, 8, 10, 11]. It is otherwise as for topography of superior oblique muscle insertion. The data reported differ greatly among themselves [8, 9, 11]. Figure 2 displays two variants (anterior and posterior) of insertion of superior oblique muscle (grey paint).
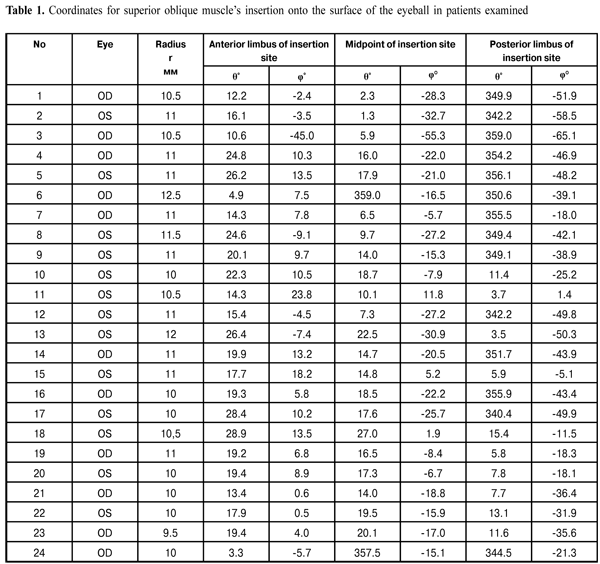
We performed the mapping of insertion sites of superior oblique muscles in twenty-four eyes of 19 patients. Table 1 presents the data on coordinates of insertion sites using SCS, in particular, anterior border of insertion site, midpoint of insertion site, and posterior border of insertion site. The term “midpoint of insertion site” is not of an exact geometrical meaning here, but an extra point on the eyeball surface where muscle’s tendon inserts; this makes it possible to localize the topography more precisely. Therefore, this point is not always just in the middle between the points of anterior and posterior borders. Narrow lines in Figure 2 illustrate sites of insertion of superior oblique tendon to the sclera (the thickness of the tendon is given not to scale). The numbers at one of the ends in these lines coincide with those in Table 1.
As seen from Table 1 and Figure 2, superior oblique muscles insertion sites are localized between 340° and 30° longitude and between 25° and -65° latitude. However, the major area of superior muscle insertion is between 350° and 25° longitude and between 10° and -50° latitude. Herewith, the anterior border of insertion is mainly located within the range between 10° and 25° longitude and posterior borders are scattered from 350° and 15° longitude. As for latitude, it is even more variable: there are both extremely anterior (No 11 and 15) and extremely posterior (No3) borders of insertion sites. The relative longitude of the insertion site is also widely ranged: from minimal (No 3, 11, 15, 18, 19, 24) to maximal (No 1, 2, 5, 14, 17) values. Of course, the variety in localization of superior oblique muscle insertion revealed cannot characterize the normal topography since all children examined had different types of strabismus. However, variable topography of superior oblique muscle insertion sites can explain great clinical variability of strabismus with lesions of superior oblique muscles. Obviously, during the evolution process, the site for superior oblique muscle insertion has not been “defined precisely” despite the rectus muscles. Conclusions The use of ophthalmographic spherical coordinate system enables to standardize the localization of superior oblique muscle insertion sites without regard to the size of the eyeball. The possible localization of the superior oblique muscle insertion to the sclera was admeasured within the range mainly between 340° and 30° longitude and 25° and -65° latitude.
References 1. Avetisov ES, Kovalevskii EI, Khvatova AV. Guidelines for Pediatric Ophthalmology. M.: Meditsina; 1987. 496 p. Russian. 2. Akimenko EV, Okunevych TA. [The relationship between eye ball size and the insertion site of extraocular muscles in 1-3-year-old children with concomitant strabismus]. [Medical and medico-pedagogical rehabilitation of children with refraction abnormalities and diseases of oculomotor system. VI scientific practical conference of pediatric ophthalmologists of Ukraine]. Lviv; 2015: 16-18. Russian. 3. Vit VV. Vit VV. [The structure of the human visual system]. Odessa: Astroprint. 2003. 664 p. 4. Yemchenko VI, Kukharenko DV, Kirilakha NG et al. [A computer programme for calculation object coordinates on the surface of the human eye]. Oftalmol Zh. 2008;4:49-52. Russian. 5. Mahkamova H. M.[ Anatomical Topographic Features of Extraocular Muscles]. Vestn. ophthalmol. 1970;78-80. Russian. 6. Kukharenko DV, Mospan VO, Yemchenko VI. Pat. 37269 UA, MPK A 61 B 3/00, G 09 B 23/00. [Method of calculating the coordinates of objects on the surface of the eyeball model]; owner — Kukharenko DV — 2008 06807; appl. 19.05.2008; publ. 25.11.2008, Bul. № 22. Ukrainian. 7. Yemchenko VI, Mospan VO, Litovchenko SO et al. [Topography of the human eye surface in spherical co-ordinates]. Oftalmol Zh. 2005;5:75-80. Russian. 8. Duke-Elder S. Textbook of Ophthalmology. V.1 St. Louis: Mosby;1941.1080 p. 9. Helveston E M. Atlas of Strabismus Surgery. St. Louis – Toronto – Princeton: The C. V. Mosby Company; 1985. 395 p. 10. Bartels M., Birch-Hirschfeld A., Cords R. Orbita. Nebenh?hlen. Lider. Tr?nenorgane. Augenmuskeln. Auge und Ohr. Berlin: Verlag von Julius Springer; 1930. 745 p. 11. Sachsenweger R. Augenmuskell?hmungen. Leipzig: VEB Georg Thieme; 1966. 463 p.
|