J.ophthalmol.(Ukraine).2016;1:12-18.
|
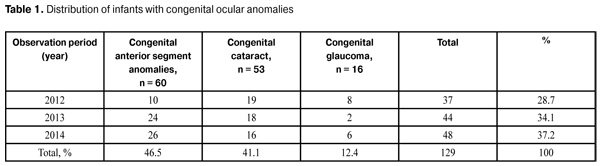
https://doi.org/10.31288/oftalmolzh201611218 Concomitant somatic disorders in infants under one year with congenital ocular anomalies N.F. Bobrova, Dr. Sc. (Med), Prof O.N. Romanchuk, pediatrician Filatov Institute of Eye Diseases and Tissue Therapy Odessa, Ukraine E-mail: filatov_detskoe@mail.ru Background: Recent studies of the clinical features and pathogenesis of the acquired, progressive and complicated myopia have evidenced that patients with this disease have reduced antioxidant defense. It is hypothesized that pharmacological correction of antioxidant defense system failure will improve visual functions in myopes. Purpose: To assess the status of visual functions (including distance visual acuity, absolute reserve of accommodation and photopic light sensitivity) in patients with myopia of different degrees before and following treatment with an antioxidant medication (Fakovit). Materials and Methods: The Fakovit treatment group included 70 myopes (140 eyes) (mild myopes, n = 28; medium myopes, n = 22; high myopes, n = 20), whereas the control group included 30 aged matched myopes who did not receive Fakovit treatment. All patients underwent ophthalmic examinations including refractometry, biomicroscopy, echobiometry, ophthalmoscopy, and absolute reserve of accommodation. The uncorrected and corrected distance visual acuities (VA) were assessed using the Shevalev’s Chart, and absolute reserve of accommodation (RA) was assessed using a conventional technique. Photopic light sensitivity was assessed with the use of semi-automatic registering adaptometer. Results: An improvement in VA was achieved in 86.1% of mild and medium myopes of the treatment group. An improvement in and stabilization of RA was found in 44.4% (mainly, in mild myopes) and 38.8%, respectively, of the patients of the treatment group, and a 1.43±1.29-D reduction in RA (p < 0.05) was observed in the control group. Photopic light sensitivity of the visual system had a tendency to increase in all myopes after treatment with Fakovit (in particular, it increased statistically significantly by 0.16±0.04 log units in mild myopes), and did not change in the controls. Conclusion: Correction of antioxidant defense system failure with Fakovit improved and stabilized visual functions (visual acuity, reserve of accommodation, and photopic light sensitivity) in myopic patients. Key words: infants, congenital fetal malformations, cataract, glaucoma, intrauterine infection Introduction Child health protection is an important current medical, social and state issue and involves a set of tasks aimed at reducing the perinatal and child mortality rates, promoting health of children at different life stages and preventing child disability, congenital and hereditary diseases from occurring [1, 2]. Somatic disorders are the most common cause of disability in children, followed by central nervous system (CNS) and sensory organ disorders, and congenital malformations and anomalies. Congenital fetal malformations (CFM) are one of the most dangerous complications of pregnancy and a leading cause of death and disability among infants. According to the WHO Expert Committee, population rate of congenital malformations and anomalies is 1.5% to 5% (with 2.7% to 16.3% variations in some countries), with the prevalence of 40-60/1000 live births [3]. According to Pokanevich [4], the mean prevalence of congenital, including hereditary disorders among newborns in Ukraine during 1993 to 2001 period was 26.31/1000 live births. CFM form a wide polyetiological group of ontogenetic disorders caused by teratogenic exposure, chromosomal abnormalities and gene mutations. The most common teratogenic agents are fetal exposure to unfavorable environmental factors (chemicals, medications and radiation), viral and bacterial infections (measles, rubella, herpes, cytomegalovirus, Toxoplasma and Chlamydia), hereditary load of gene and chromosomal mutations and their combinations. However, at least 25% of CFM cases are idiopathic [2, 5-8]. These are sporadic birth defects which are not likely to occur in future children. The purpose of the study was to analyze concomitant somatic disorders in infants under one year with congenital ocular anomalies. Materials and Methods We retrospectively analyzed the medical records (In-patient Medical Record, f.112/u recording form) of 129 infant patients under one year with congenital ocular anomalies who were treated at the Pediatric Ophthalmic Department of the Filatov Institute from 2012 to 2014. The following data were taken into account: any history of extragenital or obstetric disorder of the mother, pregnancy and labor course, child’s gestational age and health status, results of laboratory (complete blood count, urinalysis, blood biochemistry, immune status, TORCH markers, and stool analyses) and instrumental (neurosonography, electroencephalogram, electrocardiogram, sonography of internal organs and brain MRI) examinations, and considerations reported by subspecialists (neurology, cardiology, otorhinolaryngology and pediatrics). Mean infant patients age was 6.25 ± 2 months, with a range of 1/2–12 months. Results and Discussion We registered different congenital malformations of the anterior segment (abnormalities of eye size and corneal size (microphthalm, mircocornea and macrocornea), and changes in iris structure and color (heterochromia and coloboma)), congenital cataract and congenital glaucoma in infants under study. The yearly number of ocular abnormal infant patients visiting the clinic showed a tendency to increase (Table 1) from 37 (28.7% of the study group) in 2012 to 44 and 48 (34.1% and 37.2%) in 2013 and 2014, respectively. Most likely, this was not only due to advances in diagnostic techniques but also due to an actual increase in the number of infants with different congenital (including ocular) malfunctions. Visualized anatomic anterior segment anomalies (changes in eye size and corneal size such as microphthalm, mircocornea and macrocornea; changes in iris structure and color such as heterochromia and coloboma) were the most common reason (60 infants; 46.5%) for visit to the clinic. Altered lens transparency (cataract) was found in 53 infants (41.1%). Sixteen infants (12.4%) visited the clinic for congenital glaucoma.
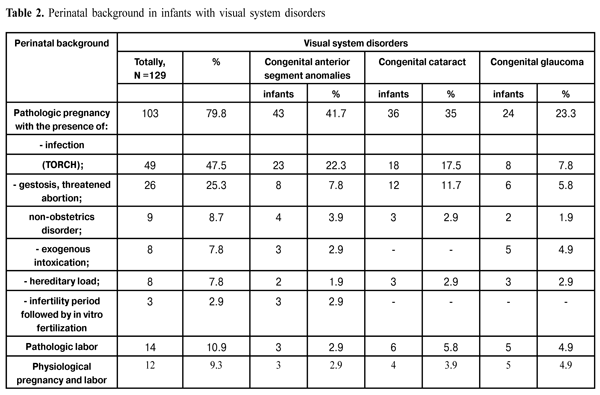
The in utero developmental period is the most important stage of the organogenesis. Several critical embryonic and fetal developmental stages are identified during which the germ is highly susceptible to different unfavorable environmental factors. The first critical embryonic developmental stage is during the first 14-15 days of fetal life when cell differentiation and formation of germ layers and extraembryonic tissues take place. The developing embryo responds to the environmental exposure according to the all-or-nothing principle. It either dies or continues to develop perfectly normally due to its high reparative capability. The second critical developmental stage is during gestation weeks 3-8, when the most important organs are formed. Additionally, at this stage, severe congenital fetal malformations (those of the neural tube, heart, vascular system, skeletal system and kidneys) are formed. These malformations are called embryopathies and are found in 13% of embryos; in most of such cases, a pregnancy terminates in a miscarriage. The CFM formed since gestation week 9 (the third critical developmental stage) are called fetopathies and are characterized by hypoplasia of different organs and the fetus at large; in such cases, a pregnancy terminates in a miscarriage or results in the birth of a malformed fetus. Teratogens are internal and external environmental factors that can cause defects, cell death and alteration in cell differentiation in the developing embryo. Teratogenic exposure at different stages of embryogenesis may result in an alteration in the morphological differentiation of multiple organs and structures (and alteration in the morphogenesis of ocular structures in particular) [9, 10]. We retrospectively analyzed the health status and labor course of mothers of infants with congenital ocular anomalies. The following perinatal risk factors were taken into account: any history of extragenital or obstetrical disorder of the mother, viral and/or bacterial infections of any etiology during pregnancy, aggressive external factors (exogenous intoxication), pathologic pregnancy (gestosis, threatened abortion) and labor course, and a hereditary load. Table 2 presents the analysis of perinatal background of infants with congenital ocular anomalies. One hundred and three infants (79.8%) with visual system defects were born after complicated pregnancies with fetal exposure to aggressive external or internal factors. Viral and bacterial agents played a rather important role in the development of CFM of different organs. Viral infection had been detected during pregnancy in 49 women (47.5%). In 9 women, acute or exacerbation of chronic TORCH infection was present during pregnancy.
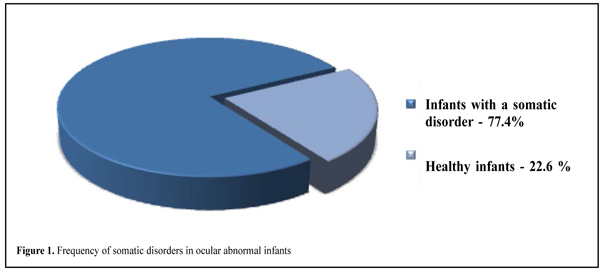
It is well known that transmission of infection to the embryo or fetus can occur via the transplacental route. Additionally, pathogen reproduction can occur in the cells of the reticuloendothelial system, nerve tissue, and ocular tissues, resulting in multisystem infectious processes. The selective nature of damage of internal fetal organs by different infectious agents with the development of a set of symptoms specific to each infection should be noted. In the study reported, herpetic viral infections were the most common teratogenic infectious agents, with cytomegalovirus having the most aggressive influence on the fetus. CMV antibodies showed the highest frequency (and were found in 41.5% of the infants under study), followed by antibodies to HSV-1 and HSV-2 (26.4%), rubella (5.7%) and Epstein-Barr virus (3.8%). The role of bacterial agents was also significant. Thus, congenital toxoplasmosis was found either predominantly or only in ocular structures in 17% of the infants, whereas the role of Chlamydia in the development of a congenital ocular malformation was proved in 1.9% of the cases. Threatened abortion at any stage of gestation can be considered a marker of the development of congenital fetal malformation. According to the data presented, in pregnancies of 26 women (25.3%), there was a threatened abortion or signs of gestosis of different severity. In 9 women (8.7%), an extragenital disease (a disease of cardiovascular, urinary or endocrine systems such as obesity, diabetes mellitus, and connective tissue disorder) was present during pregnancy. An exposure of a pregnant woman’s body to aggressive external environmental factors (emotional stress and/or contact with chemical products and chemicals, including heavy metal salts) was registered in 8 cases (7.8%). A hereditary congenital visual system disorder was found in 8 infants (7.8%), with hereditary congenital cataract and hereditary glaucoma found at the same frequency (3 infants) in each of the groups under analysis. In 3 mothers (2.9%) of ocular abnormal infants, the relevant pregnancy occurred after a long infertility period followed by in vitro fertilization, and hormone correction was used through the entire course of pregnancy. An abnormal labor course (uterine inertia with the following labor stimulation or aggressive labor management; long-term dehydration with the risk of fetal bacterial infection; accelerated labor) was observed in 14 cases (10.9%). Since no fetal exposure to teratogenic or mutagenic agents was noted in 19 mothers (9.3%) of ocular abnormal infants, and their labor was physiological, the birth defect in those infants could be considered as sporadic. Out of 129 ocular abnormal infants of the study, 110 infants (85.3%) were full-term (including 15 babies (13.6%) being small for gestational age (intrauterine growth retardation syndrome)) and 19 infants (14.7%) were pre-term. The most significant role of teratogenic prenatal factors was in the development of congenital anterior segment anomalies (Table 2; 41.7% of cases). Congenital cataract and congenital glaucoma developed in 35% and 23.3%, respectively, of cases with prenatal disorder. Out of 129 ocular abnormal infants of the study, 100 infants (77.4%) were diagnosed with a concomitant somatic disorder, and 29 infants (22.6%) were found to have neither malformation nor malfunction of internal organs (Fig. 1).
Not only the period of the fetal exposure (a critical period of the embryogenesis) to the teratogenic agent, but also the exposure time, teratogen dose and the maternal and fetal genetic constitution are important for the development of CFM. Table 3 presents the spectrum of somatic disorders found in association with congenital ocular anomalies in infants under study. The central nervous system (CNS) injury was the leading concomitant somatic disorder (51.8%), mainly due to hypoxic and traumatic perinatal CNS injuries resulting in the development of disorders of cerebrospinal fluid (CSF) flow dynamics and motor disorders of different severity (and even the development of pareses, paralyses, or convulsive disorder) (42.4%). This was caused by a reduction in the resistance of the brain of the infant to teratogenic intranatal factors following exposure to intrauterine aggression.
Congenital brain malformations were diagnosed in 13 cases (9.4%), including manifestations of hydrocephaly, microcephaly, neuronal migration disorder and brain and cerebellar hypoplasia in 8 cases, 2 cases, 1 case and 2 cases, respectively. Cardiovascular system examination revealed 46 cases of structural cardiovascular (CVS) disorders in infants of the study. Dysplastic alterations (tricuspid and mitral insufficiency with regurgitation, patent foramen ovale, anomalous trabeculae in heart cavities) were identified in 36 cases (25.9% of total cases of concomitant somatic disorders). Hemodynamically significant congenital heart disease (CHD) and vascular anomalies (ventricular septal defect, interatrial septal defect, transposition of vessels, and complete atrioventricular septal defect) were diagnosed in 10 cases (7.2%), including 2 cases associated with cardiac conduction system damage and cardiac rhythm disturbances. In 7 cases (5%), congenital ocular anomalies were involved into a genetic defect (Down syndrome or amino acid metabolism abnormality). It has been reported [11,12,13] that a chromosomal aberration may be caused by altered immune reactivity (dysimmunoglobulinemia and increased levels of circulating immune complexes with teratogenic effect). Four congenital genitourinary abnormality cases (2.9%) were related to renal malposition, malformation, and/or urinary tract dilatation, and involved 2 cases associated with genital organ malformation. Congenital locomotor abnormalities, mostly maxillofacial injuries (congenital palatal fistula, oblique facial cleft) and hip joint dysplasia were registered in four cases (2.9%) and were associated with congenital abnormalities of eye size and ocular structures. Congenital respiratory tract abnormalities were found in 1 infant of the study. With the coincidence in terms of differentiation of fetal organs and tissues, interaction of different mutagenous, teratogenous and embryotoxic factors at different stages of ontogenesis can result in the development of multiple congenital anomalies. Multiple congenital anomalies including disorders of different organs and systems with concomitant ocular injury were observed in 17 out of 100 infants with somatic disorders. The most frequent were the combinations of congenital abnormalities of the CNS and CVS. Developmental abnormalities of heart vessels and cavities were registered in 9 infants with congenital brain malformations (microcephaly, hydrocephaly, brain and cerebellar hypoplasia, structural brain abnormalities). Multiple internal organ anomalies were observed in infants with chromosomal aberration (Down syndrome and amino acid metabolism abnormality, 6 infants and 1 infant, respectively). Thus, brain injuries were associated with CHD (complete atrioventricular septal defect, ventricular septal defect, interatrial septal defect) and underactive thyroid function (hypothyroidism) in infants with trisomy 21 (Down syndrome) of the study, and the development of CNS, CVS and osseous system defects was observed in an infant with amino acid metabolism abnormality. The data presented demonstrate that anterior segment and lens abnormalities were most frequently associated with CNS injuries and CVS injuries. Thus, association of anterior segment and lens abnormalities with CNS injuries and CVS injuries was observed in 38 cases and 15 cases, respectively. Congenital cataract was associated with CNS injuries (24 cases) and CVS injuries (19 cases), whereas associations of congenital ocular anomalies with other internal organ system abnormalities were less frequent. Congenital brain malformations (leukomalacia, cortical dysplasia, microcephaly, brain and cerebellar hypoplasia, developmental abnormalities of the CSF tract) diagnosed result in the development of severe dysfunctions accompanied by motor disorders and world perception abnormality. Anatomic and functional defects of internal organs and a perinatal CNS injury with the development of disorders of CSF flow dynamics of different severity especially, contribute to the development of cerebral circulation, dystrophic, edematous-and-hemorrhagic abnormalities which exacerbate the pre- and post-operative courses and affect the outcome of surgery for correction of ocular disorder. Furthermore, delayed psychomotor development following CNS injury affects perception and analysis of visual images and, consequently, eventual functional outcome. Presence of a severe congenital cardiovascular abnormality and cardiac conduction system damage determines the term for surgical correction of structural ocular abnormality, and this is also bound to affect eventual functional outcome. Congenital respiratory and genitourinary system abnormalities accompanied by functional defects, especially if secondary infection is present concomitantly with hypoxic tissues, chronic bacterial and endogenous infection, create unfavorable conditions for reconstructive surgeries. A study similar to this was performed at the Pediatric Ophthalmic Department of the Filatov Institute in 2009 [14]. One hundred infants aged 1 to 24 months with congenital cataracts had been included in the surveillance cohort. It was demonstrated that perinatal CNS injury (66.3%) was the most common somatic disorder in infants with congenital cataracts. Cardiovascular abnormalities were registered in 19.3% of cohort infants. Additionally, the role of intrauterine infection in the development of congenital CNS and ocular abnormalities was noted. Determination of “baseline” health status of infants less than one year with congenital ocular anomalies was the feature of the study reported here. The study demonstrated that congenital CNS abnormalities were the leading somatic defect (51.8%) caused by exposure to pre- and intranatal aggressive factors. However, severe motor disorders that can be diagnosed only in older age (infantile cerebral paralysis and cognitive dysfunction) were not taken into attention. The increasing role of viral and bacterial infections in the development of congenital CNS abnormalities of multiple organs (including the eye) is of special note. In the study reported here, the involvement of intrauterine infection in the development of congenital ocular anomalies was proved in 47.5% of cases. Additionally, the role of hereditary load in the development of congenital glaucoma and congenital cataract should not be underestimated. It has been reported [15] that association with heredity was proved in 33% of cases of births of infants with congenital glaucoma and congenital cataract. Conclusion First, a concomitant somatic disorder was diagnosed in 77.4% of ocular abnormal infants, with a congenital ocular anomaly most commonly associated with those of the CNS (51.8%) and CVS (33.1%). Second, it was demonstrated that in 17% of ocular abnormal infants, given the coincidence in terms of differentiation of fetal tissues, the exposure to different mutagenous, teratogenous and embryotoxic factors at different stages of embryogenesis resulted in the development of multiple congenital anomalies. Our findings point to the need to check-up the women of reproductive age comprehensively, with involvement of immunological, genetic, and general clinical examinations, and a set of sanitation measures to minimize the risk of birth of a child with congenital abnormalities.
References 1. Ormantayev KS, Habizhanov BKh, Mashkeev AK. [Analysis of current status and tendencies of development of world and national pediatric science]. Izvestiia NAN RK. 2011; (3). Russian 2. Baranov AA, Scheplyagina LA. [Current issues of fundamental and applied pediatriсs]. Rus Pediatr J. 2005;3:4-7. Russian 3. World Health Organization. Congenital anomalies. Fact sheet N°370. In: Media centre. World Health Organization, Geneva; 2014. http://www.who.int/mediacentre/factsheets/fs370/en/. Accessed 10 Jan 2015. 4. Pokanevych TM. [Risk factors for the development of congenital abnormalities among newborns (based on the data of genetic monitoring of Kyiv region population)]. [Cand. Sc. (Med) Thesis]. Kyiv: Marzeev Institute of Hygiene and Medical Ecology; 2003. 23 p. Ukrainian 5. Shah DM, Boehm FH. Fetal blood gas analysis from cordocentesis for abnormal fetal heart rate patterns. Am J Obstet Gynecol. 1989 Aug;161(2):374-6. 6. Zaporozhan VM, Napkhaniuk VK, Kholodkova EL. [Early human embryogenesis and potential mechanisms of development of congenital abnormalities]. Visn Probl Biol Med. 2000;1:15-23. Russian 7. Demikova NS, Kozlova SI. [Monitoring of congenital abnormalities]. Vestn RAMN. 1999;11:29-32. 8. Zaporozhan VN, Serdiuk AM, Bazhora IuI et al. [Hereditary diseases and congenital abnormalities in perinatal practice: Tutorial]. Kyiv: Zdorov’ia;1997. 360 p. Ukrainian 9. Vit VV. [Structure of human visual system]. Odessa: Astroprint; 2003. 665 p. 10. Bobrova NF, Vit VV. [Atlas of congenital and hereditary ocular disorders]. Odessa: Palmira; 2006. 140 p. 11. Barnashev IuI. [Perinatal medicine and child disability]. Akush Ginek (Moscow). 1991;1:12-8. Russian 12. Sopko NI, Gaidai GL, Chernyshov VP et al. [Tumor necrosis factor and its soluble receptors in amniotic fluid of pregnant women in congenital abnormalities of the fetus and placenta]. Perinat Pediatr. 2000; 3:11-3. 13. Shabaldin AV, Glushkov AN, Kazakova LM et al. [Immunological markers of congenital fetal CNS anomaly]. Pediatriia. 2003;1:19-23. 14. Bobrova NF, Dembovetskaia AN, Zhekov AK. [Concomitant disorders in infants under two years with congenital cataracts]. Oftalmol Zh. 2009;1-2:63-69. 15. Rykov EM, Savina SA. [Current issues of ophthalmogenetics in Ukraine]. Tavr Med Biol Vestn. 2013;16(3):177-84.
|