J.ophthalmol.(Ukraine).2016;1:3-7.
|
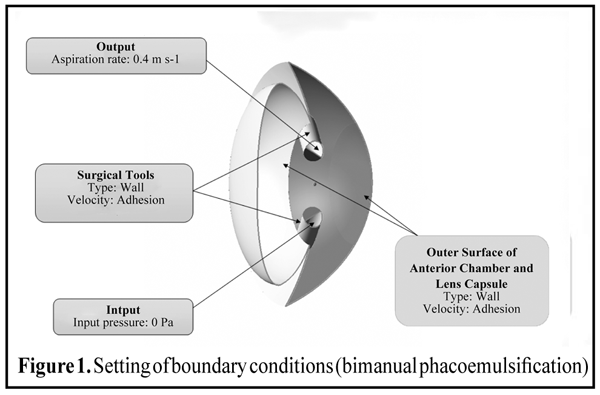
https://doi.org/10.31288/oftalmolzh2016137 Optimization of cataract phacoemulsification methods with phakic intraocular lenses D.O. Marshava1, Doctor, D.Sh. Sichinava2, Professor 1 Multiprofile clinics L/J; Kutaisi (Georgia) 2 Chavchavadze Tbilisi State University; Tbilisi (Georgia) E-mail: marshava-david@mail.ru Introduction. Development and advancement of bilensectomy technique are essential, since the number of implanted phakic IOL is rising every year. Purpose. To optimize the location of surgical instruments during phacoemulsification of the eyes with phakic intraocular lenses. Material and methods. The work is dedicated to the simulation of liquid flows in ocular anterior chamber when performing bilensectomy. A few types of cataract phacoemulsification for an eye not operated before and an eye with implanted phakic IOL were considered. Results. Washing time was set for bimanual and coaxial phacoemulsification as well as for coaxial phacoemulsification with PIOL. The integral rate in the central part of cornea (a measure of friction force) was 0.0032 m/s and 0.0015 m/s in the bimanual and coaxial surgery, respectively. Conclusion. The data received allow pursuing further studies in this area that provides increasing of efficacy and bilensectomy safety. Key words:cornea, phakic intraocular lenses, phacoemulsification, computer simulation Introduction The number of implantations of different types of phakic intraocular lenses (PIOL) has increased in the last decade. Over the past 10 years, according to various literature sources, the number of implanted different models of phakic intraocular lenses in the world has ranged from 10 to 25 thousand. At present, about 1-3 thousands of various models of PIOL are implanted every year [7, 9, 10]. Despite for a small share of total refractive surgery, PIOL have occupied their niche in the correction of myopia over 15.0 D, hyperopia from 5 to 13 D, including in children and teenagers [1, 13]. The publications on the development of cataract in different terms after PIOL implantation have appeared in national and foreign literature as more data of long-term results of PIOL implantation become available [5, 11]. In 2000 J. Colin suggested the term "bilensectomy" (BEC), which meant the surgery of simultaneous removal of PIOL, extraction of natural lens with opacity and implantation of aphakic lens [8]. In the national and foreign scientific publications available to us, we found works just stating a fact of cataract development in the eye with PIOL and the need to carry BEC [6,12]. So, the development and advancement of bilensectomy technique is essential. This work is dedicated to the simulation of a washing stage of eye during the cataract surgery by bimanual phacoemulsification and cataract surgery by coaxial phacoemulsification. When using coaxial phacoemulsification, the cases with an eye not operated before and with implanted PIOL were considered. The purpose of the study is to optimize the PE technique in the patients with cataract developed after implantation of phakic intraocular lenses. Material and Methods At the first stage of work, a physical model of washing liquid flow was developed to prevent the damage of cornea endothelium in phacoemulsification. The washing liquid is viewed as an incompressible viscous medium under the conditions of steady flow. This assumption is true even with fluctuations in discharge of washing liquid in a wide frequency range. Frequency ?, from which non-steady wave processes should be considered, can be evaluated by the formula: where c is sound velocity in washing liquid, L is a typical size of flow range. Applies to an eye: L =10 mm. Thus, threshold value ? is at least 105 Hz and the considered processes fall within this range. One phase addressed was the rinsing liquid with parameters similar to the parameters of intraocular fluid: density ?=1000 kg/m3, viscosity v=0.014 Pa [2]. Reynolds number was calculated to check that the flow is not turbulent: Where Re= ? is fluid density, V is flow velocity, v is a coefficient of dynamic viscosity, L is typical size. In case of washing fluid discharge L is a diameter of tube, which can reach up to 3 mm. Then, Reynolds number will not exceed 90 that is less than critical value Re=2 300, common for the flows in tubes. Consequently, washing fluid flow is a laminar. In case of emulsion flow in surgical field, the value L has the value about 10 mm, then Re=300, which is as well far from threshold value. So, there are only laminar fluid flows. Differential equations of Navier-Stokes, which describe the hydrodynamics of the studied flows, were used. They are worked with numerical techniques taking in consideration boundary conditions. As a result, required parameters of the flow will be defined (pressure, velocity) in different points of the studied area. In this work a program complex FlowVision HPC [4] was used, with the help of which laminar flow of viscous ocular fluid has been simulated. Irrigation and aspiration surgical instruments were used in the method of bimanual phacoemulsification. Setting of boundary conditions is shown in Figure 1. A type of boundary "wall" with a boundary condition for velocity named "adhesion" (i.e. it's equal to zero) is set on the surface of the first camera, crystalline lens, surgical instruments. Differential pressure 0 Pa (calculated based on the absolute pressure equal to 101000 Pa) is set on the end surface of irrigation device. Pumping rate 0.4 m/s is set on the end surface of aspirating device.
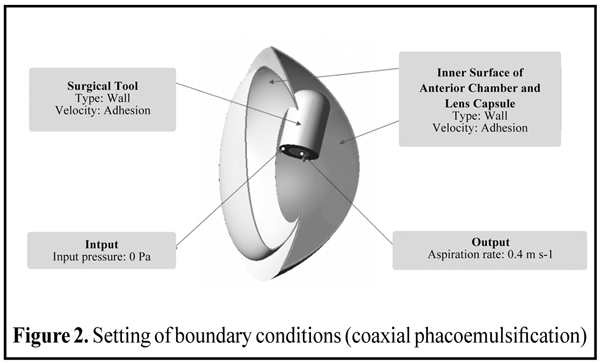
In coaxial phacoemulsification method, the surgical instrument with coaxial tip is used in which the functions of fluid aspiration and irrigation are combined. Setting boundary conditions of a task does not differ from bimanual phacoemulsification method (Fig. 2).
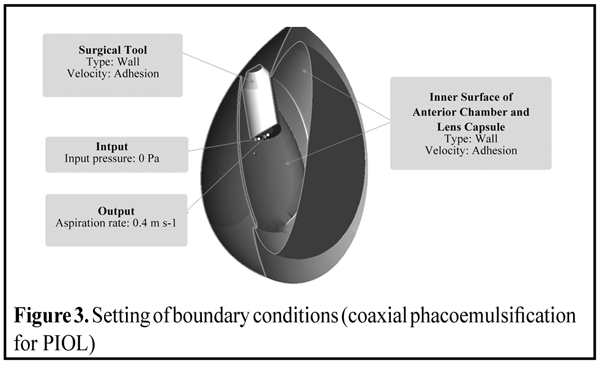
In coaxial phacoemulsification method for PIOL, the operation of eye washing by coaxial phacoemulsification method in the eye with previous implanted artificial lenses (PIOL) is considered. Setting boundary conditions does not differ from the previous cases (Fig 3).
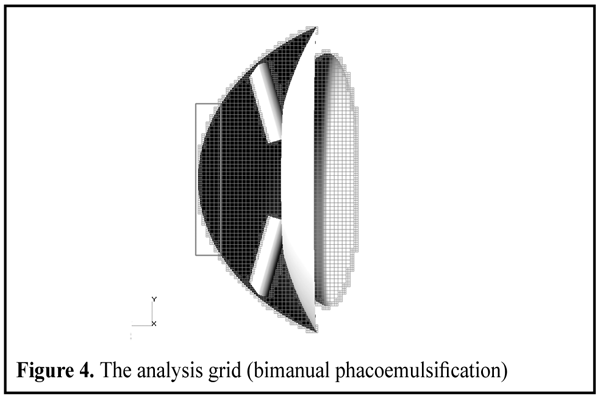
Results and Discussion In the experimental part of the work, the analysis grid used in Flowvision HPC was studied, which is orthogonal, adaptively and locally grind and with the mesh geometry of resolution. This allows to adapt cammed surfaces by rectangular meshes. In this work a certain initial mesh was regenerated, which then was adapted in the points of variable high graduents. The study of mesh convergence was conducted. Different levels and number of layers of adaptation were addressed. The mean pressure in the central part of cornea was used as convergence criterion for the grid. So, the number of computational cells in bimanual phacoemulsification turned to be equal 123 877, and in coaxial phacoemulsification with and without implanted lens it was 188 882 and 155 149 cells, respectively (Fig. 4).
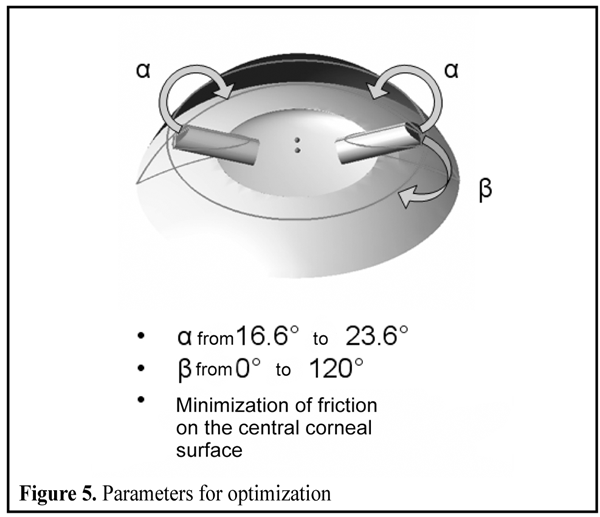
The parameters, which influenced the flow of fluid in eye, were determined with different methods of phacoemulsification. Bimanual phacoemulsification method. The simulation of flow was carried with varying of different parameters of the configuration of devices: angles perpendicular to the plane of iris; angles parallel to the plane of iris and depth of instruments penetration. Nine various situations were discussed, out of which the best and the worst positions were identified. The pressure in the central part of the cornea (against the intake pressure of fluid in irrigation device) and average velocity of the flow in the central part of the cornea (friction force in the cornea) were used as criteria for selection. The best result was obtained when the devices were symmetrically positioned and directed in the center of the lens. The worst results were obtained when the instruments were positioned at a shallow angle to each other and had various depth of penetration. Two parameters were selected for further optimization. The first parameter is an angle in the plane perpendicular to the iris plane. Both instruments will symmetrically move along it within the appropriate range. The second parameter is an angle in the plane parallel to the iris plane. It will be established at the irrigation device and vary within the preset range at the aspirator (Fig. 5).
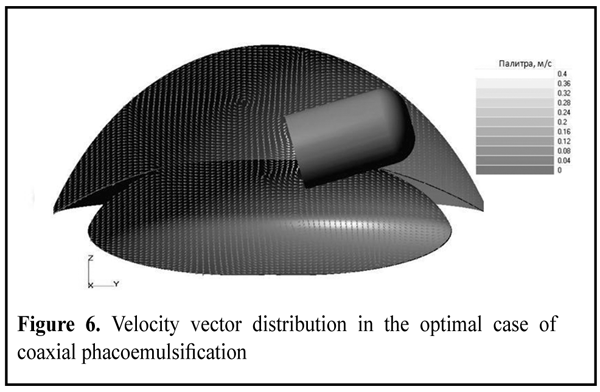
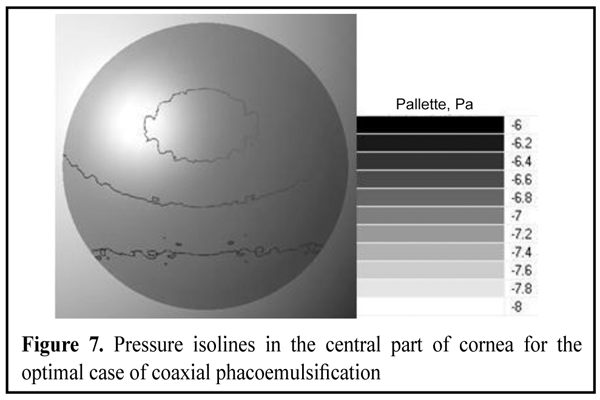
Coaxial phacoemulsification method. The simulation of flow was carried with varying of the depth of coaxial device penetration. Five various positions of the instrument were considered. The average pressure of fluid flows in the central part of cornea and the pressure in the central part of the cornea (against the intake pressure of fluid in irrigation device) were monitored. It was found that while decreasing the depth of instrument penetration, friction forces on the cornea linearly grew on the fluid side, and differential pressure sharply increased with minimal penetration depth. Velocity vector distribution in the best variant is shown in Fig. 6. Pressure isolines in the central part of cornea are presented in Fig. 7.
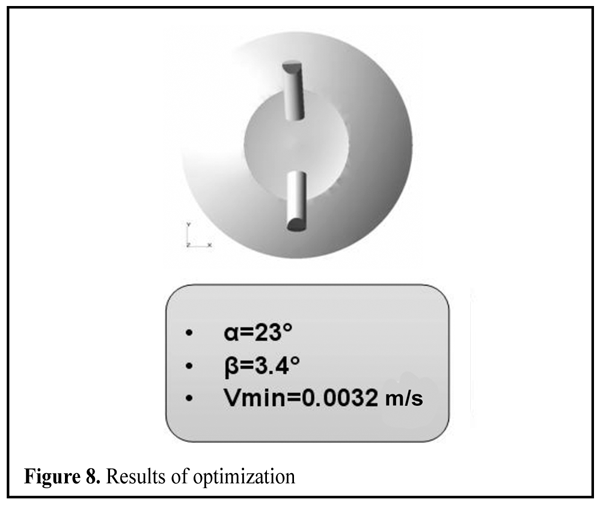
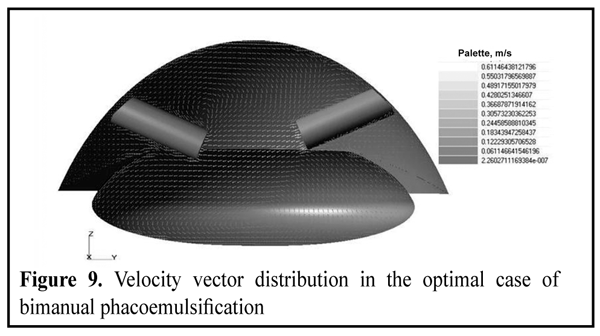
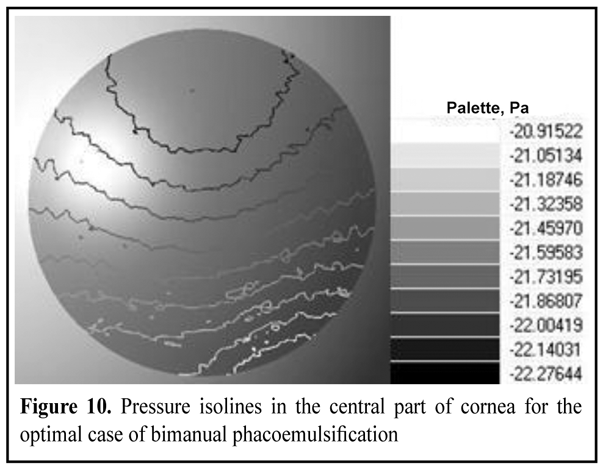
Optimization of positions of the devices in bimanual phacoemulsification. Optimization of positions of the devices in bimanual phacoemulsification were carried with IOSO NM [13] program complex according to the selected parameters and. 100 various variants were addressed and the best one from the point of the minimal average velocity of fluid flows in the central part of cornea (minimal friction force) was identified. The minimal velocity was 0.0032 m/s with the following angles: ?=23°, ?=3.4° (Fig. 8). Velocity vector distribution in the anterior chamber of the eye and pressure isolines in the central part of cornea are presented in Fig. 9 and Fig. 10, accordingly.
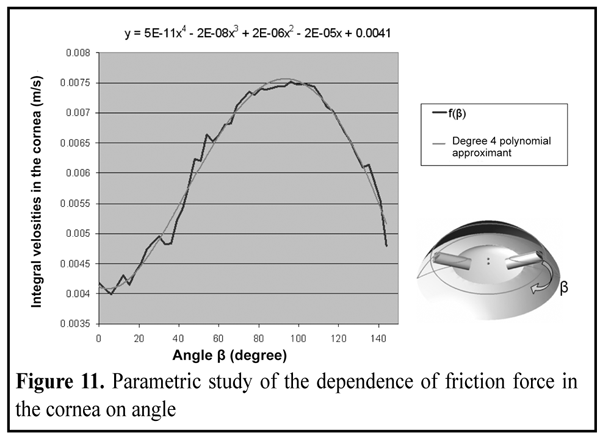
The parametric study of the dependence of an average velocity of fluid flows in the central part of the cornea on the angle (the irrigation device was fully set in the optimal position) was pursued. A specific dependence was determined. It was approximated by a polynomial of the 4th degree and the corresponding formula was received (Fig. 11).
Identification of time of irrigation — aspiration of the lens cap and the ocular anterior chamber. In this case, the study of time for irrigation and aspiration of the ocular anterior chamber as well were pursued by bimanual and coaxial phacoemulsification. Aspiration was considered to be completed when all parts of the study area (anterior chamber and lens cap) were filled with irrigation fluid, i.e. they were completely washed. The study proved that the time of irrigation and aspiration in bimanual phacoemulsification equated 554 seconds, while in the coaxial phacoemulsification (a case without lens) ? 771 seconds. The actual duration of the irrigation and aspiration was many times smaller (120 - 300 seconds) as with the complete washing of the lens cap surgery was usually completed in order to avoid traumatic effects on the rear cornea epithelium, and in the case of coaxial phacoemulsification surgical instrument was rotated manually for aspiration of difficult sites. The case of coaxial phacoemulsification for PIOL, in which the lens cap and the areas of eye difficult to irrigation and aspiration was completely washed within 832 seconds, was considered as well. Irrigation fluid penetrated into the anterior chamber, where at a time of washing did not reach the central area of the cornea. The coaxial method is currently a widely used method of phacoemulsification. If you select this method, the key factors are mainly fewer cuts of the cornea, possibility of adjusting the position of a surgical instrument, as well as the best indicator of the zones of high speeds in the area of the cornea [1]. When position of surgical instruments had been optimized and the best positions had been identified on the criterion of minimizing the friction forces in the central part of the cornea, it was appropriate to compare methods of bimanual and coaxial phacoemulsification. The comparison was conducted according to three criteria: integral velocity in the central part of the cornea <V> (measure of the friction force), integral pressure on the cornea <?P> calculated relative to the pressure set at the position of the opening of the irrigation tool (measure of differential pressure in eye) and eye wash duration ? as well. The results are shown in the table 1.
It was found that the use of coaxial instrument was a safer method of phacoemulsification surgery. However, it should not be forgotten that this method has more difficult to wash areas that requires a large experience and dexterity of the surgeon. Conclusion The optimal positions of the instruments in irrigation and aspiration of an eye during phacoemulsification through a three-dimensional numerical simulation were found; devices were placed symmetrically and directed to the center of the lens. It was found that the time of irrigation and aspiration in bimanual phacoemulsification equaled 554 seconds, while in the coaxial phacoemulsification (a case without lens) was 771 seconds. The case of coaxial phacoemulsification for PIOL was also considered, in which the lens cap and the areas of eye difficult to access for irrigation and aspiration was completely washed within 832 seconds. It was found that the integral velocity in the central part of the cornea (measure of friction force) in bimanual and coaxial phacoemulsification was 0.0032 m/s 0.0015 m/s, respectively. References 1. Agafonova VV. Correction of ametropy via intraocular phakic lens: Thesis of M.D. М.;2006:354. Russian. 2. Malyugin BE. Medical and technological system of surgical recuperation of patients with cataract, based on suprasonic phacoemulsification together with implantation of IOL. Thesis of... M.D. M.: S.N. Fyodorov Eye Microsurgery Interbranch Scientific and Technical Complex “Eye microsurgery”. 2002. Russian. 3. Marchenkova TE, Bubnov AV, Kholodov АS. [Mathematical modeling of irrigation and aspiration technique of phacoemulsification]. Ofthalmokhirurgiia. 1991;1:74-84. Russian. 4. Moskalev IV. [Characteristics of measurement of translating bodies with free surface in FLOWVISION HPC. General recommendations for organization and settlement]. In: Proceedings of all-Russian research and practice conference “Engineering systems-2008”. 2008:74-84. Russian. 5. Tiblevich IV. Analysis of the results of cataract extraction with one-piece intraocular lens implantation from PMMA: Thesis of M. D. М.;2001:108. Russian. 6. Brauweiler PH, Wehler T, Busin M. High incidence of cataract formation after implantation of a silicone posterior chamber lens in phakic, highly myopic eyes. Ophthalmology. 1999;106(9):1651-1655. 7. Caramello G, Di Fortunato R. Three years experience of ICL implantation in high myopia. In: Congress of the ESCRS, 16th: Abstracts. Nice. 1998. 8. Colin J. Bilensectomy: the implications of removing phakic intraocular lenses at the time of cataract extraction. J. Cataract Refract. Surg. 2000;26(1):2-3. 9. Gasser L, Biermann J, Reinhard T. New posterior chamber phakic intraocular lens for high myopia: Three-year results. Journal of Cataract & Refractive Surgery. 2015;41(8):1610–1615. 10. Gross S, Knorz MC, Liermann A et al. Results of implantation of a Worst Iris Claw Lens for correction of high myopia. Ophthalmologe. 2001;98(7):635-638. 11. Jos? F. Alfonso, Carlos Lisa, Luis Fern?ndez-Vega et al. Prevalence of cataract after collagen copolymer phakic intraocular lens implantation for myopia, hyperopia, and astigmatism. Journal of Cataract & Refractive Surgery. 2015; 41(4):800-805. 12. Kohnen T. Cataract formation after implantation of myopic phakic posterior chamber IOLs. Journal of Cataract & Refractive Surgery. 2004;30(11):2245–2246. 13. Laurence C Lesueur, Jean L Arne. Phakic posterior chamber lens implantation in children with high myopia. Journal of Cataract & Refractive Surgery. 1999;25(12):1571–1575.
|