J.ophthalmol.(Ukraine).2015;6:33-36.
|
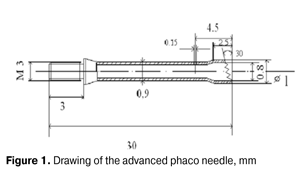
https://doi.org/10.31288/oftalmolzh201563336 Improved phaco needle for dense nucleus Ya.A. Grytsenko, MD S.K. Dmitriyev, Dr. Sc. (Med), Prof N.V. Pasyechnikova, Dr. Sc. (Med), Prof Filatov Institute of Eye Diseases and Tissue Therapy Odessa (Ukraine) E-mail: awsed2005@ukr.net Keywords: phaco needle, dense nuclei, cataract Background: Phacoemulsification (phaco) of the dense nuclear cataract tends to be associated with difficulties caused by impossibility of breaking the nucleus up completely. Therefore, the development of a phaco needle allowing for an improved capacity of ultrasound to destroy the dense nucleus with minimal ultrasound expense is important. Purpose: To improve a phaco needle for dense nucleus in order to allow for a more effective destruction (fragmentation and cutting) of the lens and aspiration of fine lens matter through a reduction in a level of lens exposure to ultrasound from the needle. Materials and Methods: Forty-six patients (50 eyes) underwent phacoemulsification with intraocular lens implantation. In 23 cases, the surgeon used the conventional phaco chop nucleus-dividing technique with the aid of an advanced phaco needle. No intraoperative complication was observed. Results: We have developed an improved phaco needle which has the following feature when compared with a conventional one: the end surface of the flared portion has a plurality of isosceles teeth, allowing the needle to penetrate the nucleus and remove the phaco debris more efficiently. The use of the needle allowed for a reduction in the level of eyeball exposure to ultrasound, thus reducing the risk of intra- and postoperative complications in patients with dense nuclear cataracts. Introduction Phacoemulsification (phaco) of the dense nuclear cataract tends to be associated with difficulties caused by (a) impossibility of breaking the nucleus up completely and (b) the need to use a rather high level of eyeball exposure to ultrasound which results in increased surgery time and intra- and postoperative complications. Thus, a number of authors have reported that the development of transitory corneal edema and corneal burns were found in 24.4% and 27.3%, respectively, of mature cataract cases, which is associated with eyeball overexposure to ultrasound with the following tissue absorption of acoustic energy and heat release [1-4]. The use of torsional ultrasound for nuclear fragmentation, combination of torsional ultrasound with longitudinal ultrasound, special nuclear fragmentation techniques and modified phaco needles are the approaches aimed at reducing the operation time in an especially dense nucleus. Most of phaco needles are similar in basic structure. A conventional phaco needle is cylinder shaped and has an attachment portion, a tubular body portion, and a lumen spanning a length of the needle. The attachment portion includes a threaded end and the components for engaging and disengaging a handpiece. To improve aspiration of lens matter, the tubular portion may have a flared end portion. The latter typically terminates in a bevel end surface which forms an oval-shaped impact surface at the intersection with the tubular portion of the needle [5]. Phaco tips have variable beveled angle between 0°, 30°, 45° and 60° and a standard inner diameter of 0.9 mm or 1.2 mm. With the adoption of minimally invasive sutureless surgery, there have been reported attempts to minimize the diameter of the tubular portion of the phaco needle in order to reduce the risk of intraocular aberrations and to improve the control over the course of surgery. However, from the other hand, there have been reported cases of phaco needle occlusion in dense nucleus, resulting in increased surgery time and number of manipulations in the anterior chamber. The needle wall thickness may vary along the needle to improve aspiration of lens material [5]. A disadvantage of currently used phaco needles is a rather large area of contact between the end surface (i.e., the edge) of the needle and the nucleus, requiring an increased force for the needle to penetrate into the nucleus. The inventors of some specific types of phaco needles have tried to remove the disadvantage by changing the end surface which contacts the lens. Zaleski [6] (1997) invented a phaco needle with a tip which flat end surface includes a beveled, or stepped cutting edge. Gravlee [7] (1996) developed a phaco needle having acute cutting edge angles of the needle tip, with these angles made by beveling the inner and outer cylindrical surfaces of the tubular portion. However, that phaco needle design had varying geometry parameters of the blade along the end cross-section and an extending cutting edge. These disadvantages prevent force required for a phaco needle to penetrate the lens from being reduced substantially. Consequently, fragmentation efficiency will not be improved, and lens matter will not be fine enough to allow for efficient aspiration. The needle tip modifications above are aimed at reduction in force required for a phaco needle to penetrate the lens by providing either a smaller area of contact between the needle edge and the nucleus or a sharper cutting edge than the prior art needle tips. The disadvantages of the phaco needles above include also the presence of flat needle edge sites being perpendicular to the needle and hampering penetration of the needle into the nucleus. Since the cutting edge of those needles extends substantially, the size of lens particles cut by the needle is too big for effective aspiration. Therefore, it is still important to improve the capacity of ultrasound to destroy the dense nucleus with minimal ultrasound expense. We hypothesize that the improvement of conventional phaco needles for dense nuclei may be aimed at reducing an area of contact between the needle edge and the nuclear tissue by providing additional cutting edges at the end surface of the needle. The purpose of the study was to improve a phaco needle for dense nucleus in order to allow for a more effective destruction (fragmentation and cutting) of the lens and aspiration of fine lens matter, through a reduction in a level of lens exposure to ultrasound from the needle. Materials and Methods We retrospectively analyzed the records of examination and surgical treatment of 46 patients (50 eyes; age, 64 to 84 years) with mature senile cataract who underwent phacoemulsification with intraocular lens (IOL) implantation. Patients with a cataract complicated by a concomitant ocular disorder were excluded from the study. Patients were divided into two groups of 23 individuals (25 eyes) each. The same surgeon performed all surgeries by the conventional phaco chop nucleus-dividing technique with the Infiniti system and identical ultrasound parameters. A main corneoscleral tunnel incision made with a 2.2 mm keratome was routinely used. Patients of Group 1 were operated using an advanced phaco needle, and patients of Group 2 were operated using a conventional phaco needle (INTREPID® Micro-Coaxial System). The mean cumulative dissipated energy (CDE) was automatically calculated and displayed on the monitor of the Infinitі phaco system intraoperatiotively. Preoperational examinations included the following: lens density measurement involving ultrasound B scanning (20 MHz B-scan transducer, Quantel Medical Cinescan S) with determination of lens echogenicity [8], in accordance with an advanced methodology (Patent of Ukraine No. 93206); biomicroscopy; assessment of visual acuity (VA); and direct assessment of corneal endothelial cell density. Postoperatively, patients were administered conventional medication therapy involving antibacterial and anti-inflammatory agents and corneal regeneration stimulators, and were followed up for 1 to 3 months. Preoperative VA was 0.01 to 0.1 and light perception with accurate light projection in 6/50 eyes (12.0%) and 44/50 eyes (88.0%), respectively. Since the ultrasound examination revealed that the relative acoustic impedance of the lenses was 0.28 to 0.36 units, these lenses can be classified as mechanically hard. Clinically, all study eyes with senile cataract were classified as those having grade 4 nuclei and grade 5 nuclei (Buratto classification scheme). Statistica 8.0 and Microsoft Excel 2013 software were used for statistical analysis and assessment of the significance of results. Data were presented as mean and standard deviations. P values < 0.05 were considered significant. Results and Discussion We have patented an improved phaco needle (Patent of Ukraine for the useful model No. 64851) which has the following feature when compared with a conventional one: the end surface of the flared portion has a plurality of isosceles teeth along the oval-shaped impact surface, with a tooth height exceeding the amplitude of axial needle vibration, and a tooth pitch allowing the aspirated lens matter to be allocated in between the teeth (Fig. 1).
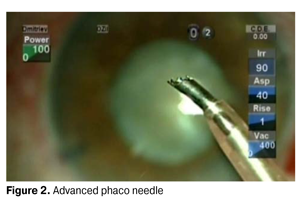
Increased efficiency of lens destruction occurs because the geometrical parameters (edge angle; thickness; height) of the cutting portion of a tooth are now approximately the same as those of another tooth, and, consequently, these cutting portions have approximately the same operating parameters during phaco ultrasound movement of the tip (forward and backwards). (Fig. 2).
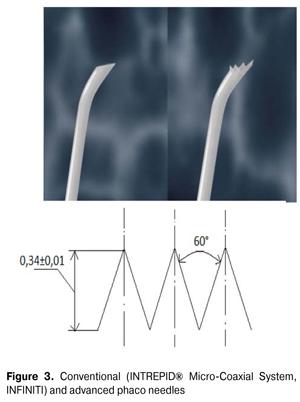
During operation of the needle, the contact of flat surfaces oriented perpendicular to motion of the needle with lens matted is excluded. Here traditional cutting blade geometry (namely, wedge-shaped geometry) which is optimal for cutting and fragmentation is utilized (Fig. 3).
The advantages of the phaco needle developed are as follows: the contact of flat surfaces oriented perpendicular to the needle motion is excluded; traditional cutting blade geometry (namely, wedge-shaped geometry) which is optimal for cutting and fragmentation is utilized. Postoperative VA in Group 1 and Group 2 was 0.37±0.02 vs 0.12±0.03 at days 1 to 3. At months 1 to 3, VA in Group 1 was noted to be improved to 1.01 ± 0.03. Corneal burns were observed in 4/25 eyes (16.0%) of Group 1 in the early postoperative period, requiring application of an additional corneoscleral suture. Diffuse corneal edema and corneal burn of different grades at the site of main incision were revealed in 9/25 eyes (36.0%) of the controls, requiring for an extension of the rehabilitation period. No intraoperative complication was observed. The mean CDE in Group 1 was 25.40 ± 1.03 units vs 36.25 ± 2.45 units in Group 2, with a statistically significant difference between the groups. Preoperatively, the mean corneal endothelial cell density in Group 1 was 2623 ± 325 cell/mm2 vs 2590 ± 341 cell/mm2 in Group 2. Postoperatively, the mean corneal endothelial cell density Group 1 was 2489 ± 275 cell/mm2 vs 2233 ± 367 cell/mm2 in Group 2. The average endothelial cell loss in Group 1 was 5.1±1.2% vs 13.7±4.3% in Group 2 (Table 1). Fuchs' dystrophy was not found in any of the groups.
In conclusion, we have developed an improved phaco needle which has the following feature when compared with a conventional one: the end surface of the flared portion has a plurality of isosceles teeth along the oval-shaped impact surface, allowing the needle to penetrate deep layers of a high-density nucleus more efficiently. The use of this needle allowed us to reduce the risk of early postoperative edema and corneal burns by 20% by reducing mean cumulative dissipated energy values. References
|