J.ophthalmol.(Ukraine).2020;2:60-64.
|
http://doi.org/10.31288/oftalmolzh202026064 Received: 21 February 2020; Published on-line: 30 April 2020 Effect of irrigation solution temperature on the duration of intraocular bleeding during vitrectomy (experimental study) R.E. Nazaretian, Junior Research Scientist, O.S. Zadorozhnyy, Cand Sc (Med), M.M. Umanets, Dr Sc (Med), V.A. Naumenko, Dr Sc (Med), Prof., N.V. Pasyechnikova, Dr Sc (Med), Prof., Corr Member of NAMS of Ukraine Filatov Institute of Eye Diseases and Tissue Therapy, NAMS of Ukraine; Odesa (Ukraine) E-mail: rudolph.naz@gmail.com TO CITE THIS ARTICLE: Nazaretian RE, Zadorozhnyy OS, Umanets MM, Naumenko VA, Pasyechnikova NV. Effect of irrigation solution temperature on the duration of intraocular bleeding during vitrectomy (experimental study). J.ophthalmol.(Ukraine).2020;2:60-64. http://doi.org/10.31288/oftalmolzh202026064
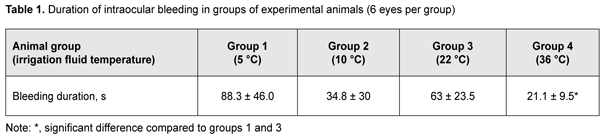
Background: Bleeding in vitreoretinal patients during and early after vitrectomy is still a challenge that needs to be addressed. Purpose: To assess the effect of irrigation fluid temperature on intraocular bleeding time in rabbits during vitrectomy. Material and Methods: Twelve Chinchilla rabbits (24 eyes) were included in this study and divided into four groups of 3 animals (6 eyes) each based on vitrectomy irrigation fluid temperature: group 1 (5° C), group 2 (10° C), group 3 (22° C), and group 4 (36° C). The ambient operating room temperature was between 22 °С and 24 °С. Results: The duration of intraocular bleeding in groups 1, 2, 3 and 4 was 88.3 ± 46.0 s, 34.8 ± 30 s, 63 ± 23.5 s, and 21.1 ± 9.5 s, respectively. Conclusion: In a rabbit model of intraocular bleeding, use of irrigation fluid of 36 °С (i.e., conditions of mild hypothermia) resulted in shorter intraocular bleeding in the perioperative period of vitrectomy compared to conventional use of room-temperature irrigation fluid (21.1 ± 9.5 s against 63 ± 23.5 s). Mild hypothermia may be recommended for use in vitreoretinal surgery in patients with a high risk of bleeding. Keywords: vitrectomy, irrigation fluid temperature, rabbit eye, intraocular bleeding
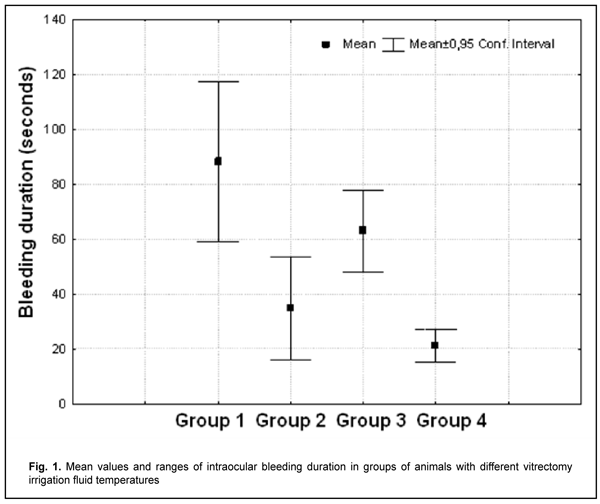
Introduction Pars plana vitrectomy is widely used in the treatment of rhegmatogenous retinal detachments, proliferative diabetic retinopathy and other vitreoretinal disorders. The surgical intervention (e.g., in severe proliferative diabetic retinopathy) is often time consuming for the performing surgeon [1]. Despite continuous advances in vitrectomy technology, there still remain a wide range of challenges that need to be addressed [2-8]. One of these challenges is bleeding in vitreoretinal patients during and early after vitrectomy [9]. The temperature of irrigation solutions used during vitrectomy is commonly lower than that of the intraocular media, and neither of these temperatures is commonly monitored during the procedure [10]. Consequently, vitrectomy is performed under conditions of uncontrolled local ocular hypothermia. Although there is no uniform protocol to administer hypothermia in intraocular surgery, some authors believe it reasonable to use low-temperature irrigating fluids to facilitate neuroprotection during vitrectomy [11-13]. In addition, currently, there are no clear recommendations on irrigation fluid temperature modes reducing the risk of bleeding during vitrectomy. The purpose of the study was to assess the effect of irrigation fluid temperature on intraocular bleeding time in rabbits during vitrectomy. Material and Methods Twelve Chinchilla rabbits (24 eyes; weight, 2.5-3.5 kg) were included in this study and divided into four groups of 3 animals (6 eyes) each based on vitrectomy irrigation fluid temperature: group 1 (5° C), group 2 (10° C), group 3 (22° C), and group 4 (36° C). The ambient operating room temperature was between 22 °С and 24 °С. A 23-G three-port pars plana vitrectomy was performed using the Alcon Accurus 400VS vitrectomy system (Alcon Laboratories, Fort Worth, TX). Technique The surgical site was prepared with antiseptic solution and epibulbar anesthetic was administered. Thereafter, core and peripheral vitrectomy was performed with cutting rates of 1500-1800 cuts/min, aspiration pressure of 150 mm Hg, and irrigation pressure of 20 mm Hg. After vitrectomy, irrigation fluid circulation was maintained for 5 minutes to stabilize intraocular temperature [11]. Thereafter, the major retinal vessels running through the medullary bundles closely located nasally or temporarilly to the optic nerve were cut to induce intraocular bleeding [9, 14, 15], and the period from cutting the vessel (and the onset of bleeding) to complete arrest of bleeding from the damaged vessel was recorded. Irrigation and aspiration were not discontinued during this period. BSS PLUS® (Alcon) was used as an intraocular irrigation fluid. Cool (5 °С or 10° С) fluid was prepared by cooling the solution inside the irrigating tube with cooling gel packs. Room-temperature (22 °C) fluid was obtained by placing the bottles with solution in the operating room for several hours before surgery. Warm (36 °С) fluid was prepared by warming the solution inside the irrigating tube with gel packs that were located outside the tube, and thus warming was performed in close proximity to the surgical site. The temperature of the irrigation fluid delivered into the eye was monitored and controlled during surgery. A thermoelectric device [18] developed by the Institute of Thermoelectricity of the NAS of Ukraine and MES of Ukraine, and the Filatov Institute was used for measuring irrigation fluid temperature. All animal experiments were performed in compliance with the Law of Ukraine on Protection of Animals from Cruel Treatment No. 3447-IV dated 21.02.2006 and European Convention for the Protection of Vertebrate Animals Used for Experimental and Other Scientific Purposes from the European Treaty Series (Strasbourg, 1986), and approved by a local Bioethics Committee of the Filatov Institute. The animals were housed and bred conventionally. Each animal underwent biomicroscopy and ophthalmoscopy before surgery and the next day after surgery. In addition, rectal temperature measurements were made before surgery and before anesthesia. Prior to surgery, animals were anesthetized with thiopental sodium 10% (1.0 mL/kg, intramuscularly). Immediately thereafter, both eyes received a drop of proxymetacaine HCl (0.5%) for topical anesthesia. The pupils were dilated with atropine sulphate. After surgery, a drop of sulfacyl natrium 20% and a drop of Ofloxacin 0.3% were applied to each operated eye immediately after surgery and four times daily for 5 days thereafter. The experimental temperature data was subjected to statistical analysis. Data is presented as mean ± standard deviation (SD). Statistical analyses were conducted using Statistica 10.0 (StatSoft, Tulsa, OK, USA) software. The level of significance p ? 0.05 was assumed. Results No change in the cornea was observed, and the lens was clear during the surgical procedure. There was no significant difference in operation room temperature or baseline rectal temperature among the groups. Mean intraocular bleeding durations for the groups are presented in Table 1 and Figure 1.
Bleeding duration was significantly (p=0.000) shorter in rabbits with a vitrectomy irrigation fluid temperature of 36 °С (group 4) than in those with a vitrectomy irrigation fluid temperature of 22 °С (group 3) or 5 °С (group 1). There was no significant difference (p=0.14) in bleeding duration between animals of group 4 and those of group 2 (irrigation fluid temperature of 10 °С). Discussion Vitrectomy is usually performed in patients who already have ischemic retinal injury, e.g., patients with diabetic retinopathy. In addition, IOP increase and systemic arterial pressure decrease during vitrectomy can result in decreased perfusion pressure, leading to additional intraoperative ischemic retinal and optic nerve injury [7]. As currently there is no classification for assessing the severity of eye tissue hypothermia, we were guided by the classification used in critical care intensive therapy units. Hypothermia can be classified based on the depth of cooling from a normal body temperature of 37-38°C: mild hypothermia (34-35.9 °C), moderate hypothermia (32-33.9 °C), intermediate hypothermia (30-31.9 °C), and deep hypothermia (< 30 °C) [17]. Mild hypothermia is known to have a positive effect on the structure and function of neural tissue under ischemic conditions. Mild hypothermia prevents blood–brain barrier disruption and its downstream effects under cerebral ischemic conditions [18], inhibits pro-inflammatory brain tissue responses [19], and suppresses cellular apoptosis [20]. Although mild therapeutic hypothermia (a reduction of a patient’s core temperature to 34.0 - 35.9 °C) has been successfully applied in critical care practice for improving brain cell resistance to ischemic conditions [17, 20], to our knowledge, only animal studies have been reported on the effect of hypothermia on the ocular cells and tissues. Intraocular temperatures undergo changes in the course of vitrectomy depending on irrigating fluid temperature. We have previously demonstrated [21] that, intraocular temperature decreased by 1°С with the use of 36°С irrigating fluid during vitrectomy (i.e., surgical interventions were performed under conditions of mild hypothermia). There has been histological evidence of apparent vacuolization of retinal structures at the microscopic slides from rabbit eyes that underwent vitrectomy under conditions of deep hypothermia, but not prolonged vitrectomy under conditions of mild hypothermia [22]. In the current study, duration of intraocular bleeding was significantly shorter in rabbits with a vitrectomy irrigation fluid temperature of 36 °С than in those with a vitrectomy irrigation fluid temperature approximately equal to room temperature (22 °С). It has been reported that hypothermia does not begin to affect platelet function until temperature decreases below 35 °C; clotting factors are affected only when temperature decreases below 33 °C [17]. Therefore, conventional conditions under which vitrectomy is commonly performed (i.e., with the use of room-temperature irrigation fluid) are not the best for efficient perioperative hemostasis. In addition, duration of intraocular bleeding was shorter in rabbits with a vitrectomy irrigation fluid temperature of 10 °С than in those with a room- temperature irrigation fluid, which is in agreement with previous findings [11]. Moreover, in the current study, rabbits with a vitrectomy irrigation fluid temperature of 5 °С exhibited the longest intraocular bleeding duration. Therefore, since mild hypothermia exerts a number of positive effects on neural tissue structures, does not result in cold-related damage to retinal tissue, and causes a reduction in duration of bleeding in the perioperative period, we find it reasonable to recommend it for prolonged vitreoretinal surgery, especially in patients with a high risk of bleeding (e.g., those with proliferative diabetic retinopathy). Conclusion In a rabbit model of intraocular bleeding, use of irrigation fluid of 36 °С (i.e., conditions of mild hypothermia) resulted in shorter intraocular bleeding in the perioperative period of vitrectomy compared to conventional use of room-temperature irrigation fluid (21.1 ± 9.5 s against 63 ± 23.5 s). Mild hypothermia may be recommended for use in vitreoretinal surgery in patients with a high risk of bleeding.
References 1.Shishkin MM, Yuldasheva N.M. [Intravitreal injection of angiogenesis inhibitors as a stage of sparing vitreoretinal surgery of proliferative diabetic retinopathy]. Bulletin of the Pirogov National Medical and Surgery Center. 2011; 6(1):77-81. Russian. 2.Farah M, Maia M, Rodrigues EB. Dyes in Ocular Surgery: Principles for Use in Chromovitrectomy. Am J Ophthalmol. 2009;48(3);332-40. 3.Goto A, Inatani M, Inoue T, Awai-Kasaoka N, Takihara Y, Ito Y, et al. Frequency and risk factors for neovascular glaucoma after vitrectomy in eyes with proliferative diabetic retinopathy. J Glaucoma. 2013;22(7):572-6. 4.Hasumura T, Yonemura N, Hirata A, Murata Y, Negi A. Retinal Damage by Air Infusion during Vitrectomy in Rabbit Eyes. Invest Ophthalmol Vis Sci. 2000 Dec;41(13):4300-4. 5.Hsuan JD, Brown NA, Bron AJ, Patel CK, Rosen PH. Posterior subcapsular and nuclear cataract after vitrectomy. J Cataract Refr Surg. 2001 Mar;27(3):437-44. 6.Postel EA, Pulido JS, Byrnes GA, Heier J, Waterhouse W, Han DP, et al. Long-term follow-up of iatrogenic phototoxicity. Arch Ophthalmol. 1998 Jun;116(6):753-7. 7.Rossi T, Querzoli G, Angelini G, Rossi A, Malvasi C, Iossa M, et al. Ocular perfusion pressure during pars plana vitrectomy: a pilot study. Invest Ophthalmol Vis Sci. 2014 Dec 2;55(12):8497-505. 8.Saito K, Fukuda N, Matsumoto T, Iribe Y, Tsunemi A, Kazama T, Yoshida-Noro C, et al. Moderate low temperature preserves the stemness of neural stem cells and suppresses apoptosis of the cells via activation of the cold-inducible RNA binding protein. Brain Res. 2010 Oct 28;1358:20-9. 9.Umanets M.M. [Effect of HF electric welding (modified generator EK-300 M1) vs diathermocougulation of major retinal vessels in rabbits]. Oftalmol Zh. 2012;4:88-92. 10.Iguchi Y, Asami T, Ueno S, Ushida H, Maruko R, Oiwa K, et al. Changes in vitreous temperature during intravitreal surgery. Invest Ophthalmol Vis Sci. 2014 Apr 11;55(4):2344-9. 11.Jabbour NM, Schepens CL, Buzney SM. Local ocular hypothermia in experimental intraocular surgery. Ophthalmology. 1988 Dec;95(12):1687-90. 12.Rinkoff J, Machemer R, Hida T, Chandler D. Temperature-dependent light damage to the retina. Am J Ophthalmol. 1986 Oct 15;102(4):452-62. 13.Tamai K, Toumoto E, Majima A. Local hypothermia protects the retina from ischaemic injury in vitrectomy. Brit J Ophthalmol. 1997 Sep;81(9):789-94. 14.de Bustros S, Glaser BM, Johnson MA. Thrombin infusion for the control of intraocular bleeding during vitreous surgery. Arch Ophthalmol. 1985 Jun;103(6):837-9. 15.Lee HS, Kim SH, Kim IT. Intraocular infusate with Hemocoagulase for the control of bleeding during vitreous surgery. Kor J Ophthalmol. 1989 Jun;3(1):6-10. 16.Anatychuk L, Pasyechnikova N, Zadorozhnyy O, Nazaretian R, Myrnenko V, Kobylyanskyi R, Gavrilyuk N. Original device and approaches to the study of temperature distribution in various eye segments (experimental study). J Ophthalmol (Ukraine). 2015;6:50-53. 17.Polderman KH, Herold I. Therapeutic hypothermia and controlled normothermia in the ICU: Practical considerations, side effects, and cooling methods. Crit Care Med. 2009 Mar;37(3):1101-20. 18.Yenari MA, Han HS. Neuroprotective mechanisms of hypothermia in brain ischaemia. Nat Rev Neurosci. 2012 Feb 22;13(4):267-78. 19.Deng H, Han HS, Cheng D, Sun GH, Yenari MA. Mild hypothermia inhibits inflammation after experimental stroke and brain inflammation. Stroke. 2003 Oct;34(10):2495-501. 20.Alzaga AG, Cerdan M, Varon J. Therapeutic hypothermia. Resuscitation. 2006;70(3):369-80. 21.Zadorozhnyy O, Nazaretian R, Myrnenko V, Naumenko V, Maltsev E, Pasyechnikova N. [Structure of the chorioretinal complex in the rabbit eye after vitrectomy. Report 2. Vitreous cavity irrigation with different temperature solutions for 60 minutes]. J Ophthalmol (Ukraine). 2018;4:49-55. 22.Zadorozhnyy O, Nazaretian R, Naumenko V, Maltsev E, Pasyechnikova N. Structure of the chorioretinal complex in the rabbit eye after vitrectomy. Report 3. Vitreous cavity irrigation with 36°С solution. J Ophthalmol (Ukraine). 2019;5:49-55.
The authors certify that they have no conflicts of interest in the subject matter or materials discussed in this manuscript.
|