Changes in clinical condition of the eye and in parameters of cell and humoral immunity in iridocyclitis patients under the influence of anti-viral allokin-alpha
N.V. Konovalova, Dr. Sc. (Med.)
N. I. Khramenko, Cand. Sc. (Med.)
L. N. Velichko, Cand. Sc. (Med.)
A. Ia. Novik, Cand. Sc. (Med.)
SI “Filatov Institute of Eye Diseases and Tissue Therapy of the NAMS of Ukraine”
Odessa, Ukraine
Introduction. Iridocyclitis, inflammatory eye disease of the uvea, is a topical issue not only in clinical but social regard, considering its high prevalence and disability rates.
Purpose. To study changes in the clinical condition of the eye and the state of cellular and humoral immunity in iridocyclitis patients under the influence of allokin-alpha anti-viral drugs.
Material and Methods. We observed 41 patients (41 eyes) with acute and chronic iridocyclitis who underwent anti-viral allokin-alpha treatment at Inflammatory Eye Pathology Department at SI “The Filatov Institute of Eye Diseases and Tissue Therapy”.
Results. Over the treatment course we observed a significant increase in immunoregulatory index from 1.16% to 2.00%; a relative T-lymphocyte count increased from 38.2±0.5% to 63.4±1.2% and a relative CD-19 lymphocyte count decreased from 24.4% to 21.8%, which reached normal parameters at 18 days after treatment onset. The treatment resulted in VA improvement.
Conclusions. Using allokin-alpha anti-viral drug enables to raise treatment success in viral iridocyclitis patients and to improve VA against the background of inflammatory process reduction.
Key words: iridocyclitis, allokin-alpha
Introduction
Iridocyclitis is a common disease that often takes on a recurrent chracter and affects young working-age people. According to different authors, iridocyclitis is a cause of blindness in 5 - 30% and 25% cases, which determines the importance and relevance of studying pathogenesis of the disease development [8]. Over the late decades, a great number of dangerous viruses have been discovered (Ebola Virus, AIDS, Marburg virus and etc.); viruses mutate actively, recombination in the virion genome takes place and viruses become resistant to traditional therapy. Human immune system does not always manage to prevent from virus replicating in the organism; immunodeficiency develops against the background of long-term persistent viral infection. The eye is under the fire of virus attacks in patients of different age in the presence of low immune function. Over the last decade, the ratio of virus infection as an etiologic agent in endogenous uveitis development has increased. Viral infections have gained a footnote and ground in human population, affecting all organs and systems of the host and developing acute, sub-acute, and chronic forms. Today, viral infection (VI) is considered as a systemic disease of the organism [1]. Expert committee of World Health Organization (WHO) has predicted an intensive VI incidence in the current century and WHO European Bureau published a report back in 1987, in which they pointed that “… herpesvirus infections will determine the future of the viral pathology in the XXI century”. 300 000 to 500 000 people with various herpes forms seek for ophthalmic help annually, where 60 % of a total number are the patients with herpetic keratitis and iridocyclitis [6].
The role of immune response has been defined in inflammation development in the uveal tract. It is known that neutrophils and macrophages migrate to the focus of inflammation in cell immunity activation (as delayed type hypersensitivity), in consequence of their activity, the reproduction of pathology causing agents is managed. The state of immune system in uveitis patients is defined considerably by immunocompetent cells’ producing cytokines that participate in formation of systemic and immune responses in different eye diseases [4, 5, 7, 10].
Recombinant interferon, the action mechanism of which consists in the possibility to induce the formation of high titre of endogenous interferons [9, 12], has been shown prospective in the uveitis treatment [2, 13]; the main producers of recombinant interferon are macrophages, T- and B-lymphocytes [14]. Taking into account these facts, it is reasonable to find out if there is a correlation between directivity and intensity of changes in cellular and humoral components of immunity when uveal tract inflammation develops and in respect of clinical signs of the disease and changes in cytokine component of immunity (due to interferon level in blood serum). Besides, immunological studies of the course of the disease will make it possible to correct pathogenic and etiotropic treatment assigned, considering the pronouncement degree of damage in every patient. Since natural killer (NK) cells are capable to control the virus spread in as little as few hours after infection, many viruses have developed the mechanisms to modulate the activity of NK cells, “hiding” from immune response activation. The necessity to use antiviral drug with immunomodulatory activity, that increases immunobiological resistance, is obvious.
Allokin-alpha is an antiviral drug, one of a new family of natural antiviral peptides, the one of Ukraine’s immunostimulant that directly activates natural killers (NK) and acts directly in the affected area not inducing immune hyperresponsiveness. It belongs to pharmacological class “Antiviral and immunomodulatory drug. Interferon inducer”.
Allokin-alpha is a synthetic linear cytokine-like oligopeptide with molecular weight of 1 265 Daltons and it consists of 13 L-amino-acids with alloferon as an active ingredient. Its action is focused on enhancement of virus antigen and infected cell recognition by natural killers, neutrophils and other natural immunity effectory systems that are responsible for virus elimination [11] and defected cell lysis by cytotoxic lymphocytes.
Purpose. To study changes in the clinical condition of the eye and the state of cellular and humoral immunity in iridocyclitis patients under the influence of allokin-alpha anti-viral drug.
Material and Methods
We observed 41 patients (41 eyes) with acute and chronic iridocyclitis that underwent inpatient treatment at Inflammatory Eye Pathology Department at SI “The Filatov Institute of Eye Diseases and Tissue Therapy”. The patients’ age averaged (38.1±13.2) y/o. Acute iridocyclitis was diagnosed in 11 patients (26.8%), chronic iridocyclitis recurrence was in 30 patients (73.2%). Virus etiology of the process was confirmed in all patients (according to the data of enzyme immunoassay (EIA), HSV1 and HSV2). All patients followed-up were divided into four groups according to visual acuity (VA) values: group i, VA < 0.1; group ii, VA between 0.1 and 0.3; group iii, VA between 0.35 and 0.6; group iv, VA between 0.7 and 1.0. Twenty healthy patients comprised a control group to compare values of cellular and humoral immunity. Clinical signs of iridocyclitis included a combined injection of conjunctival vessels, sweat corneal endothelium, precipitates on the corneal endothelium, anterior chamber exudates, posterior synechiae, intensive opacity in the vitreous, and, in 2 patients (4.8%), diffuse edema in the macular area. Intraocular pressure was within the normal range in all patients. The patients underwent treatment using allokin-alpha antivirus drug, s/c 1 mg (diluted in saline solution, 6 to 9 injection for a treatment course) every other day. The treatment was performed against the background of mydriatic atropine and phenylephrine to break posterior synechiae, and parabulbar injections of dexamethasone No 5.
Each patient was examined using a standard ophthalmic test protocol including visual acuity test, tonometry, ophthalmoscopy, visual field test, and tissue and humoral immunity studies.
Peripheral blood was studied immunologically. Parameters of T-cell immunity (T-lymphocyte population as well as subpopulations, T-helpers/inducers and T-suppressors/cytotoxic natural killers) were detected immunohistologically using CD 3+, CD 4+, CD 8+, CD 16+ monoclonal antibodies [11]. Properties of CD 16 (NK cells) to kill directly infected cells or to produce cytokines in the affected area contribute to getting virus spread under control and to virus prevalence limiting ability. Humoral immunity was assessed according to the level of b-lymphocytes (using CD 19+ donators of immunoglobulin (Ig) of various classes) and to the level of IgA, IgM, IgG using radial immunodiffusion assay (Mancini method).
The data obtained were statistically processed by Statistica 7.0 software using pairwise Student criterion and nonparametric ?2 criterion with preliminary normality test.
Results and Discussion
Changes in parameters of cellular and humoral immunity in viral iridocyclitis patients over the course of allokin-alpha treatment are given in Table 1. The inflammation onset was against the background of lymphopenia, which indicates secondary immunodeficiency and reduced immunoresistance of the organism. To assess the state of immune system, it is important to consider the state of CD-3 as a mirror reflecting pathologic processes in the diseased organism. In uveitis patients, we observed a significant decrease by 41%, р<0.05, (Table 1) in the amount of CD-3 lymphocytes in the peripheral blood, which was lower than that in control group patients. These changes evidence the apparent deficiency of a general T-lymphocyte pool in iridocyclitis patients. At 18 days after 6 allokin-alpha injections, a relative value of T- lymphocytes increased from (38.2±0.53)% up to (63.4±1.19)% (р<0.05).
СD-4 (T-helpers) are drown a special attention to in inflammatory process since these cells play an important role nearly in all immune cell and antibody-mediated responses. Various CD-4 T-cells produce different cytokine sets for humoral immune response; they are known as well as TDTH cells (delayed-type hypersensitivity T cells), cytokines for cellular immunity. Besides, HIV enters T-cell through this receptor.
T-helper count before allokin-alpha treatment was decreased (by 33.3% (р<0.05) lower than age norm). It gradually increased over the course of treatment. At 18 days after therapy start, T-helper count settled down and reached the normal values.
CD-8 is a surface molecule of the most cytotoxic T- lymphosites. T-suppressor count in all viral iridocyclitis patients was found to be higher as compared to control. This tendency was kept and T-suppressor count remained increased (by 54% higher than the norm (р<0.05)) at 18 days after treatment start.
The immunoregulatory index (IRI) (CD-4/CD-8 ratio) in the peripheral blood is diagnostically valuable and prognostic informative parameter for immune system assessment.
As it appears from the data in Table 1, IRI increased significantly from 1.16 up to 2.00 (p=0,00008) over the course of treatment, nearing the normal range at the end of treatment (Table 1).
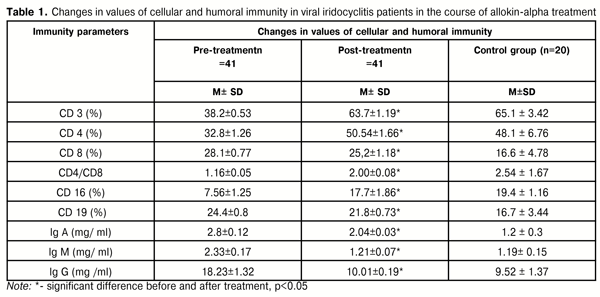
Studying the changes in CD-19 lymphocytes, we found that CD-19 lymphocyte level steady decreased from 24.4% to 21.8 % at 18 days after treatment start.
Taking into account T-lymphocyte disorders in patients examined, the ratio of main immunoregulatory subpopulations of CD-4 and CD-8 lymphocytes is of interest. We determined significant changes in relative T-helper lymphocyte count in the peripheral blood as compared to control, which indicates autoimmune shifts in the peripheral blood of patients in comparison with control group of healthy patients. Against the background of apparent T-lymphocyte deficiency, we determined a decrease in CD-4 lymphocyte proportion in the peripheral blood of viral iridocyclitis patients as compared to control group values. Besides, CD 16 (NK) count increased significantly, that enhances body resistance to viral infection.
As for humoral immunity in uveitis patients, we detected an increase in relative B-lymphocyte count and IgA level as compared to norm. IgM level was increased and, after treatment, it decreased twice with its value settling down within the normal range. IgG level in iridocyclitis patients decreased twice over the course of treatment and substantially corresponded the norm (р<0.02).
The data obtained in assessment of cellular and humoral immunity in viral iridocyclitis patients are of practical importance with the point of choice of rational pathogenically-oriented treatment including anti-virus, desensitizing and immunecorrecting therapy. All patients were prescribed allokin-alpha as anti-virus therapy and immune system correction.
Outcomes of treatment performed showed the treatment success and positive changes in the clinical picture and visual acuity. To assess the efficacy of proposed treatment in uveitis patients, we used a number of criteria and, first of all, changes in VA. VA changes against the treatment in all groups of uveitis patients are given in Table 2.
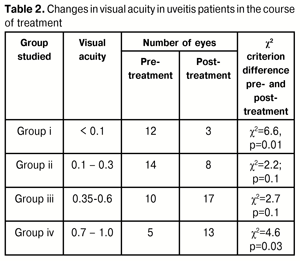
According to examination data, the number of patients with VA < 0.1 significantly decreased after treatment (p=0.01) (Table 2) due to positive changes and a VA increase up to 0.3 and higher wherefore the patients moved the group (to groups ii and iii). The number of patients of group ii with VA < 0.3 decreased since a part of patients moved to group iii (VA 0.31-0.6) and group iv (VA 0.61-1.0). A significant increase in the number of eyes with high VA was noted in group iv. Thus, visual functions were improved in all acute and chronic iridocyclitis patients, undergone allokin-alpha treatment. Clinically, in iridocyclitis, we noted exudate and precipitate resorption, posterior synechiae breaking as early as 3-5 days after treatment start. All patients underwent the treatment proposed without complication. No allergic reaction and intolerance were noted, which make it possible to introduce anti-virus allokin-alpha drug into general clinical practice.
Conclusions
1. The course of allokin-alpha treatment in viral iridocyclitis patients resulted in normalization of immune state according to cellular and humoral immunity parameters. Thus, relative T-lymphocyte count increased from (38.2±0.5%) to (63.4±1.2%) and IRI increased from 1.16% to 2.00% as well as relative CD-19 lymphocyte count decreased from 24.4% to 21.8%. The NK number increased that enhances significantly body resistance to viral infection and improves immune biological resistance of the organism.
2. Introduction of allokin-alpha into anterior uveitis treatment enables to improve VA against the background of inflammatory process reduction.
3. Due to clinical and immune benefits, the absence of allergic and other side reactions as well as favorable tolerability, allokin-alpha can be introduced into clinical practice for inflammatory eye conditions.
References
1. Barinskii IF. [Herpesviral infections - immunodeficient diseases of the XXI century. Current issues of herpesviral infections]. 2004:5-7. Russian.
2. Guliieva M. [Experimental and clinical studies of Oftalmoferon eye drops in the herpetic keratitis treatment]. Author’s thesis for Cand. Sc. (Med.). 14.00.08 Ophthalmology. M.; 2006. 30 p. Russian.
3. Degtyarenko TV. [Adaptive significance of immune homeostasis in eye diseases]. Oftalmol Zh. 1997;1:1–4. Russian.
4. Drozdova EA, Tarasova LN, Teplova SN, Alekhina TV. [Immunological features of uveitis in systemic diseases]. Vestn Oftalmol. 2004;4:24–6. Russian.
5. Zainutdinova GKh, Malkhanov VB, Shevchuk NE. [Features of systemic and local cytokine production in rheumatoid uveitis]. Tsitokiny i vospaleniie. 2008;7(2):52–5. Russian.
6. Исаков В.А. Герпеcвирусные инфекции человека / В.А. Исаков, Е.И. Архипов, Д.В. Исаков // Руководство для врачей . — СПб.:СпецЛит., 2006. — 303 с.
7. Metelitsyna IP, Levitska GV, Ghaffari Sahbi ben Mohamed Moncef. [The level of cytokines in intraocular fluids in patients with rhegmatogenous retinal detachment]. Odeskyi Med. Zhurnal. 2011; 4(126):37–9. Ukrainian.
8. Sukhina LA, Lysenko AG, Yulish ME. [Optimizing the diagnosis and treatment of chronic recurrent uveitis in children caused by persistent intracellular infections]. Oftalmologiia. Vostochnaia Evropa. 2014;2(21):20–6.] Ruaaian.
9. Khokkanen VM, Solovieva MV, Bataiev VM, Ionova OG. [Investigation of the role of cytokines in the course of tuberculous uveitis]. Collection of papers of scientific practical conference in ophthalmosurgery «East-West», 13–14 May 2011. Ufa, 2011. 350–352. Russian.
10. Shaimova VA. [The role of inflammatory cytokines in eye diseases]. (Litereature review). Oftalmokhirurgiia i terapiia. 2004;4(3):30–2. Russian.
11. Shishkin MK, Isakov VA, Iermolinko DK. Selected issues of infectious patient therapy: Guidance for physicians. SPb.: Foliant; 2005. 636-64. Russian.
12. Groot-Mijnes JDF, Groot-Mijnes L Visser, Zuurveen S et al. Identification of new pathogens in the intraocular fluid of patients with uveitis. Am. J. Ophthalmol. 2010;150 (5):628-36.
Crossref Pubmed
13. Plskova J, Greiner K, Forrester JV. Interferon-? as an effective treatment for noninfectious posterior uveitis and panuveitis. Am. J. Ophthalmol.2007;144: 55-61.
Crossref Pubmed
14. Takase H, Sugita S, Taguchi C et al. Capacity of ocular infiltrating T helper type 1 cells of patients with non-infectious uveitis to produce chemokines. Br. J. Ophthalmol.2006;90:765-8.
Crossref Pubmed